
Neonatal/Infant Resuscitation 1
Session: Neonatal/Infant Resuscitation 1
Chyi-Her Lin, MD (he/him/his)
Consultant Pediatrician
E-Da Hosp.
Tainan, Tainan, Taiwan (Republic of China)
.jpg) Interaction of panel plots among the SIRB of 280 mL or 62 mL capacity, ventilation rates (VR), and oxygen flow rates (L/min) at 20-29 cm H₂O peak inspiratory pressure over time (150 sec).
Interaction of panel plots among the SIRB of 280 mL or 62 mL capacity, ventilation rates (VR), and oxygen flow rates (L/min) at 20-29 cm H₂O peak inspiratory pressure over time (150 sec).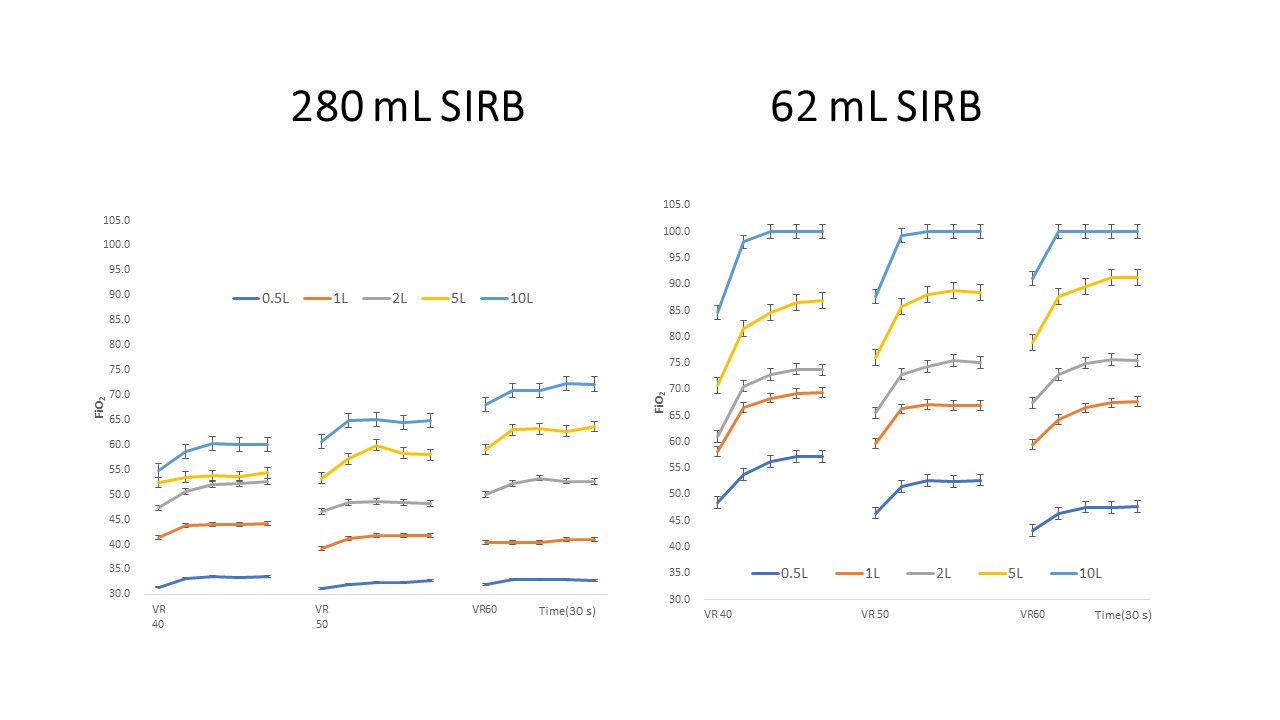 Interaction of panel plots among the SIRB of 280 mL or 62 mL capacity, ventilation rates (VR), and oxygen flow rates (L/min) at 30-39 cm H₂O peak inspiratory pressure over time (150 sec).
Interaction of panel plots among the SIRB of 280 mL or 62 mL capacity, ventilation rates (VR), and oxygen flow rates (L/min) at 30-39 cm H₂O peak inspiratory pressure over time (150 sec).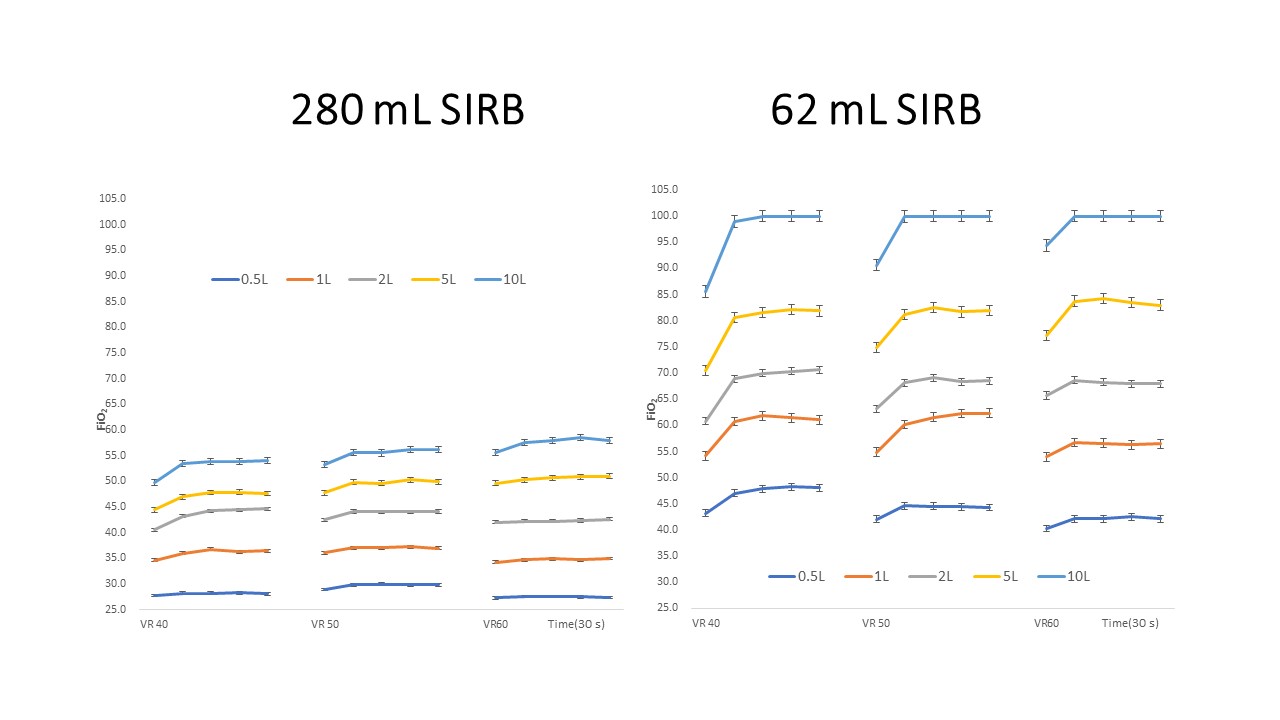 Interaction of panel plots among the SIRB of 280 mL or 62 mL capacity, ventilation rates (VR), and oxygen flow rates (L/min) at ≥40 cm H₂O peak inspiratory pressure over time (150 sec).
Interaction of panel plots among the SIRB of 280 mL or 62 mL capacity, ventilation rates (VR), and oxygen flow rates (L/min) at ≥40 cm H₂O peak inspiratory pressure over time (150 sec).