
Neonatal General 3: NICU Practices
Session: Neonatal General 3: NICU Practices
Itamar Nitzan, MD (he/him/his)
neonatologist
Shaare Zedek Medical Center
Jerusalem, Yerushalayim, Israel
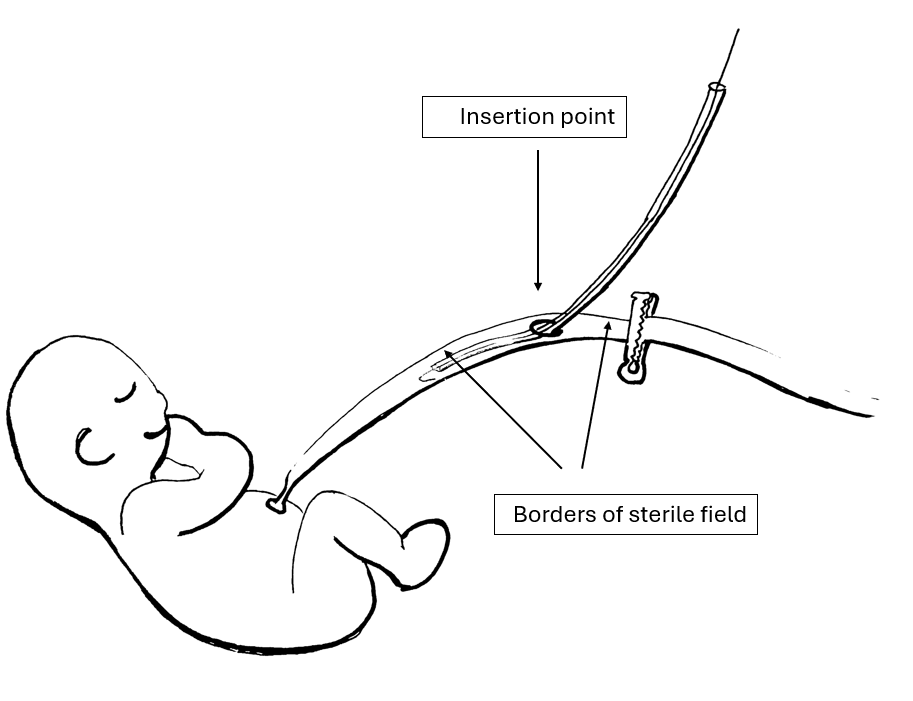 Schematic drawing of the planned method for line insertion.
Schematic drawing of the planned method for line insertion..png) Canulation of a removed umbilical cord during the study.
Canulation of a removed umbilical cord during the study.