
Neonatal General 2: Neurology
Session: Neonatal General 2: Neurology
 photo")
Terrence Lo, BMSc, PharmD, ACPR, RPh (he/him/his)
Pharmacist
The Hospital for Sick Children
Richmond Hill, Ontario, Canada
.jpg) DUE, drug use evaluation; HIE, hypoxic-ischemic encephalopathy; NICU, neonatal intensive care unit; OR, operating room; TH, therapeutic hypothermia
DUE, drug use evaluation; HIE, hypoxic-ischemic encephalopathy; NICU, neonatal intensive care unit; OR, operating room; TH, therapeutic hypothermia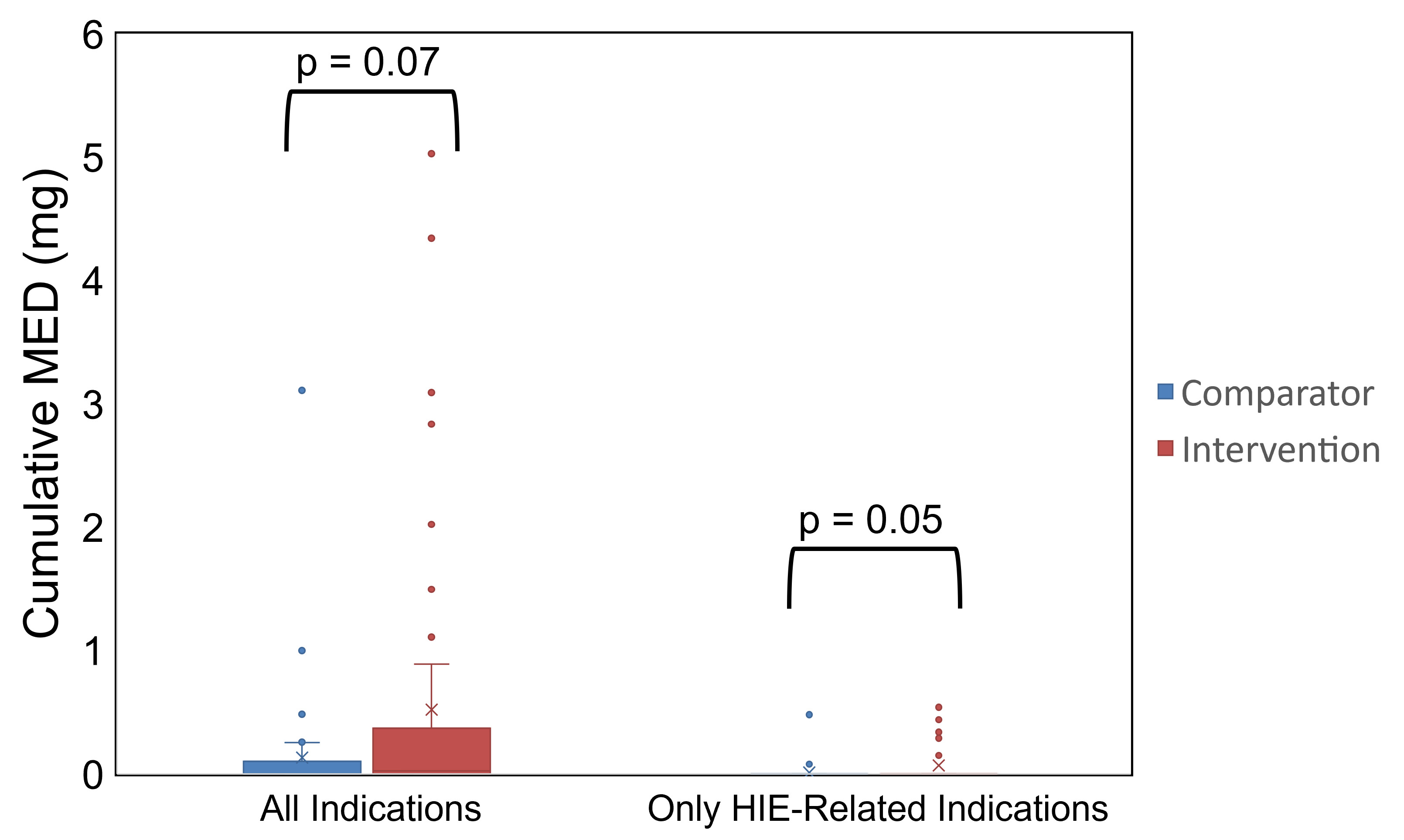 MED, morphine equivalent dose
MED, morphine equivalent dose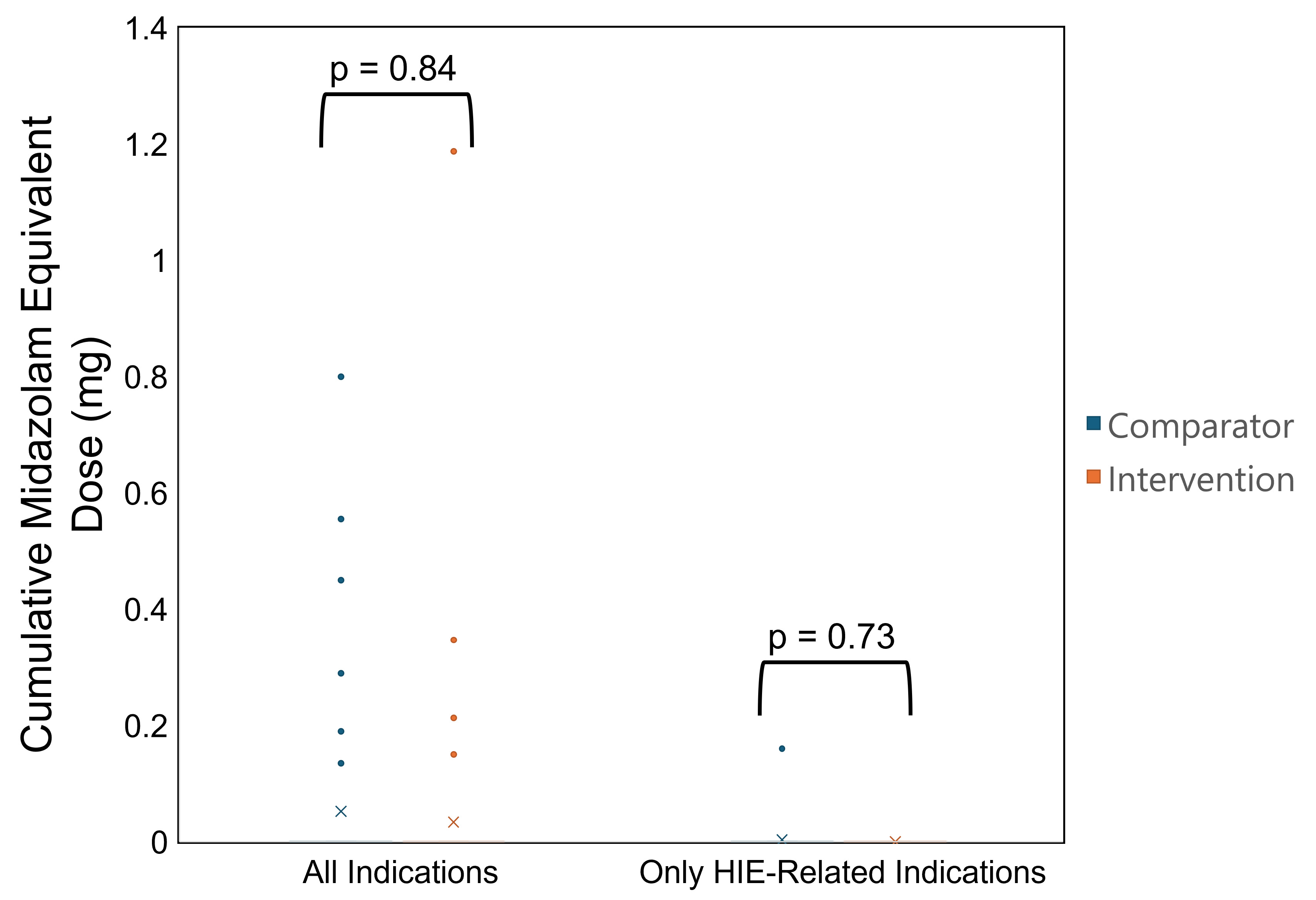 DUE, drug use evaluation; HIE, hypoxic-ischemic encephalopathy; NICU, neonatal intensive care unit; OR, operating room; TH, therapeutic hypothermiaMED, morphine equivalent dose
DUE, drug use evaluation; HIE, hypoxic-ischemic encephalopathy; NICU, neonatal intensive care unit; OR, operating room; TH, therapeutic hypothermiaMED, morphine equivalent dose