
Neonatal Neurology 3
Session: Neonatal Neurology 3
Marie Cornet, MD, PhD (she/her/hers)
Assistant Professor
University of California, San Francisco, School of Medicine
San Francisco, California, United States
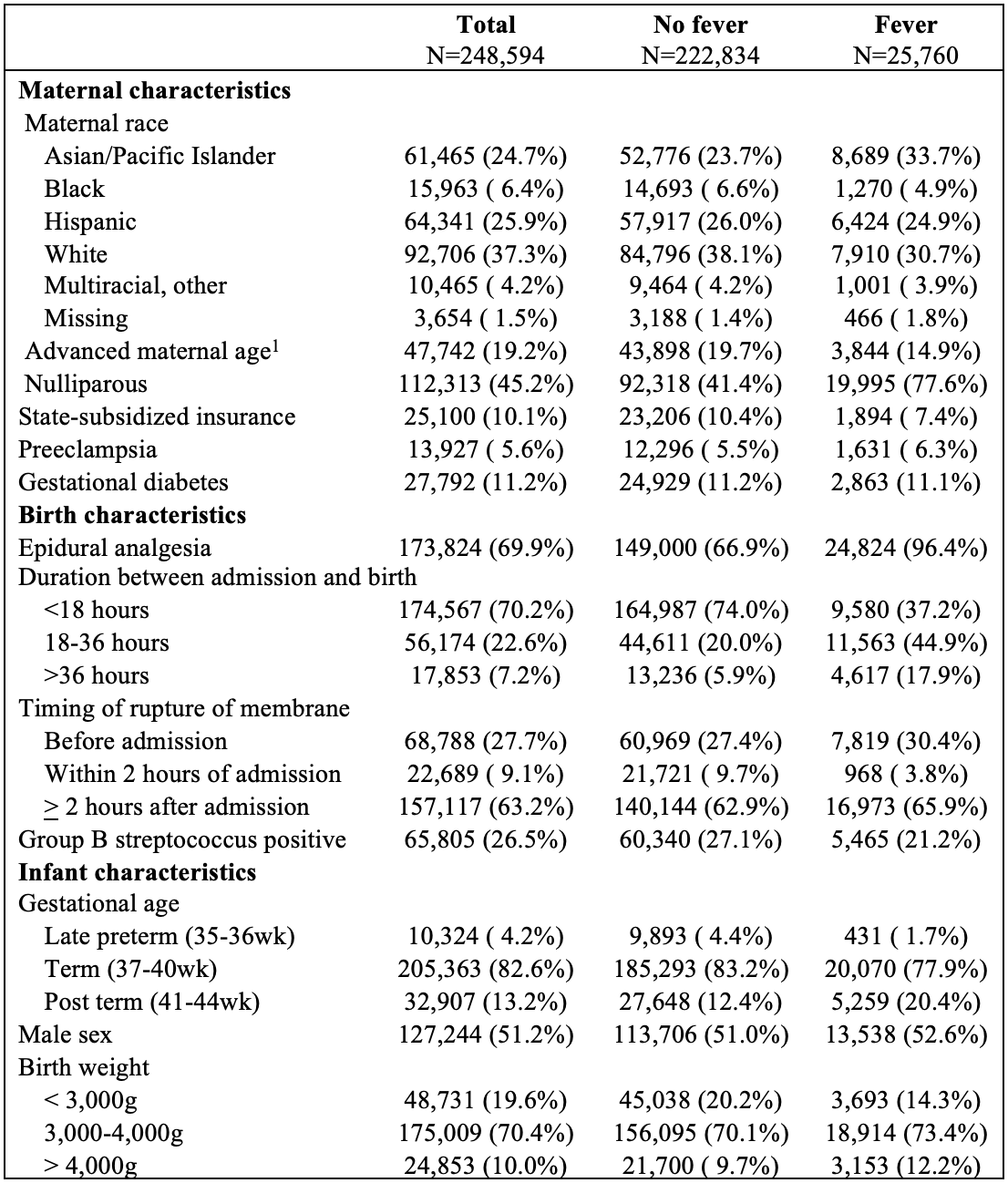 1. Maternal age>35 years old
1. Maternal age>35 years old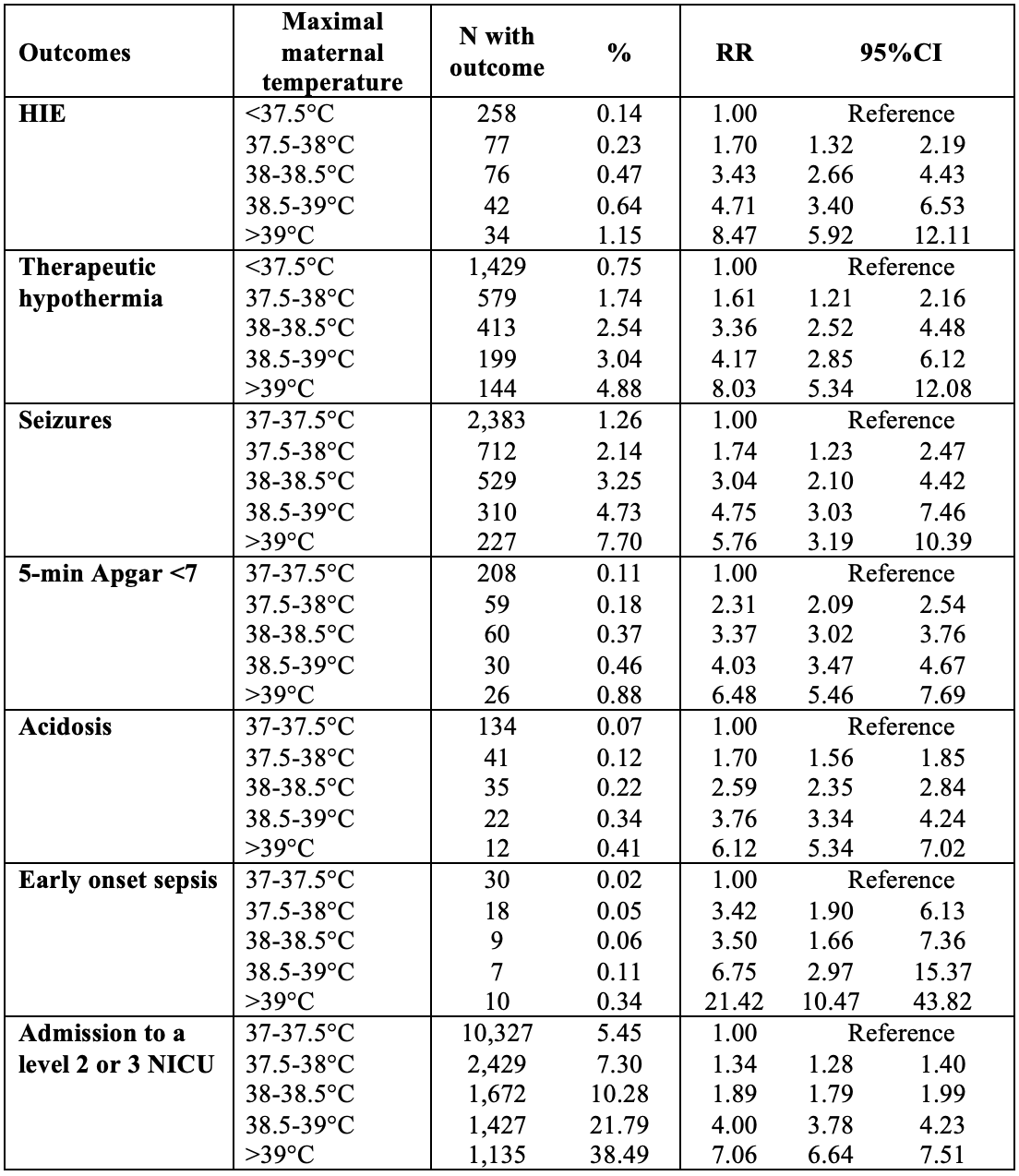 HIE: Hypoxic ischemic encephalopathy NICU: Neonatal intensive care unit
HIE: Hypoxic ischemic encephalopathy NICU: Neonatal intensive care unit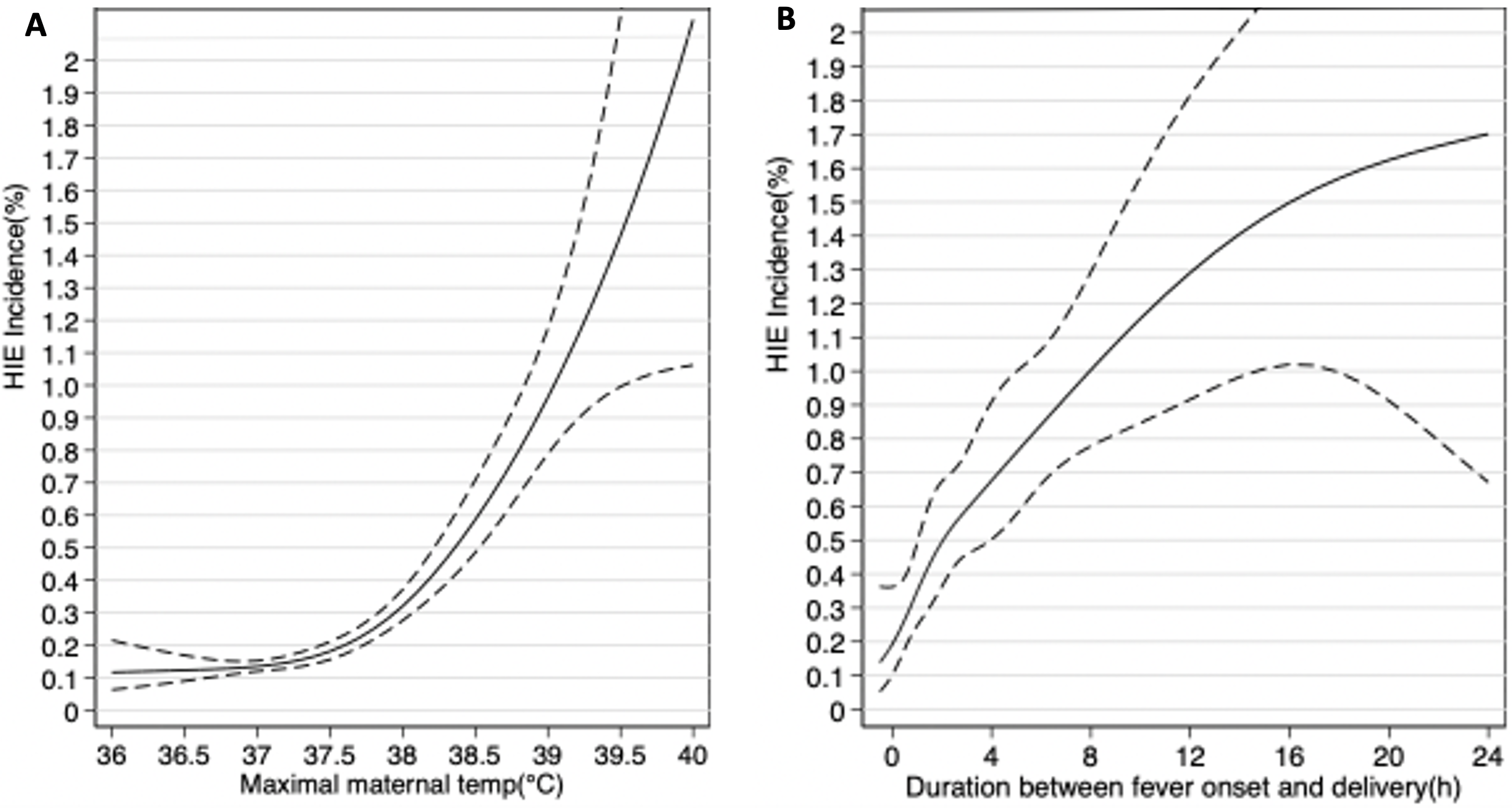 Estimations obtained by logistic regression modeling transforming predictor variables (maximal maternal temperature and duration between fever onset and delivery) as restricted cubic splines. 1. Maternal age>35 years oldHIE: Hypoxic ischemic encephalopathy NICU: Neonatal intensive care unitEstimations obtained by logistic regression modeling transforming predictor variables (maximal maternal temperature and duration between fever onset and delivery) as restricted cubic splines.
Estimations obtained by logistic regression modeling transforming predictor variables (maximal maternal temperature and duration between fever onset and delivery) as restricted cubic splines. 1. Maternal age>35 years oldHIE: Hypoxic ischemic encephalopathy NICU: Neonatal intensive care unitEstimations obtained by logistic regression modeling transforming predictor variables (maximal maternal temperature and duration between fever onset and delivery) as restricted cubic splines. 