
Neonatal/Infant Resuscitation 2
Session: Neonatal/Infant Resuscitation 2
 photo")
Rebecca Valdez, B.S. (she/her/hers)
Trainee
University of California Davis
Davis, California, United States
.jpg)
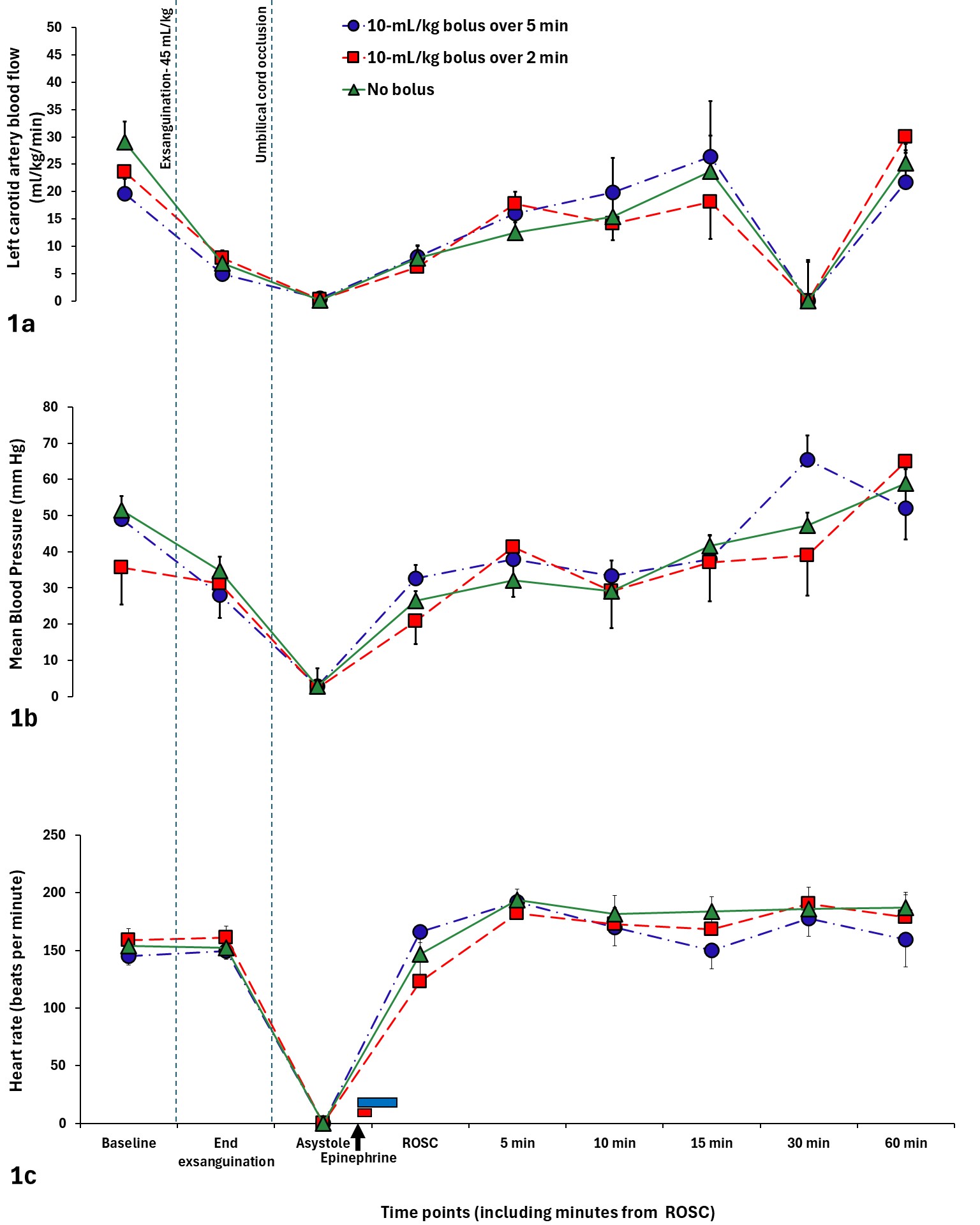 Carotid artery blood flow and mean blood pressure decreased significantly during exsanguination with no difference in heart rate. After ROSC, there was no difference in carotid artery blood flow, mean blood pressure, and heart rate between 10mL/kg normal saline bolus over 5 min vs. 2 min vs. no bolus groups. The blue bar near the x-axis represents the 10mL/kg bolus over 5 min being administered and the red bar represents the 10mL/kg bolus being administered over 2 min Data was compared using repeated ANOVA.
Carotid artery blood flow and mean blood pressure decreased significantly during exsanguination with no difference in heart rate. After ROSC, there was no difference in carotid artery blood flow, mean blood pressure, and heart rate between 10mL/kg normal saline bolus over 5 min vs. 2 min vs. no bolus groups. The blue bar near the x-axis represents the 10mL/kg bolus over 5 min being administered and the red bar represents the 10mL/kg bolus being administered over 2 min Data was compared using repeated ANOVA. .jpg)
