
Infectious Diseases 2: Bacterial infections
Session: Infectious Diseases 2: Bacterial infections
 photo")
Randal De Souza, MD (he/him/his)
Pediatric Infectious Diseases Fellow
Nationwide Children's Hospital
Columbus, Ohio, United States
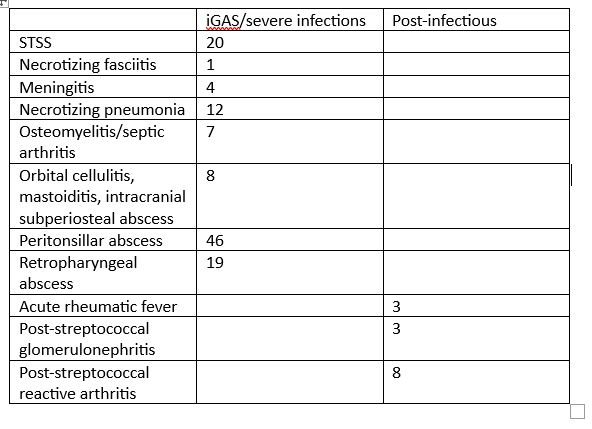 Table 1. Invasive, severe and postinfectious complications
Table 1. Invasive, severe and postinfectious complications