Neonatal Neurology 1
Session: Neonatal Neurology 1
.jpg "Lucia McLean, BSc (Hons), MD (she/her/hers) photo")
Lucia McLean, BSc (Hons), MD (she/her/hers)
Neonatal Fellow
The Royal Women's Hospital
Carlton, Victoria, Australia
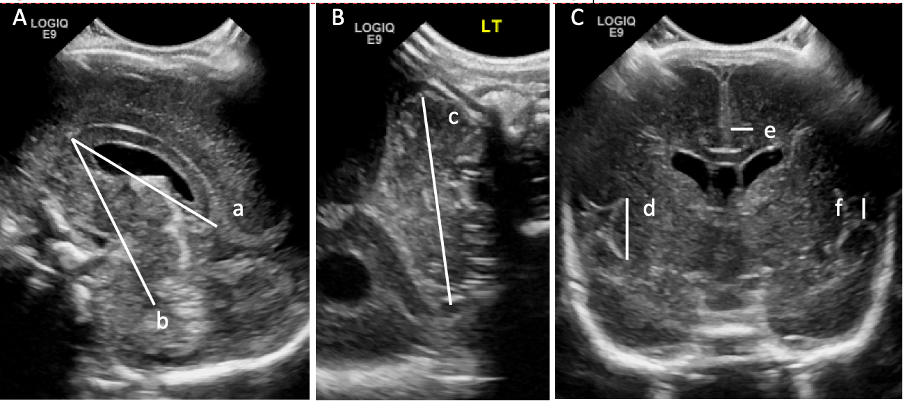 Cranial ultrasound linear measures of brain growth (A and B) and maturation (C). Images taken through the anterior fontanelle in the midsagittal plane (A) and coronal plane at the level of the foramina of Monro (C) and through the mastoid fontanelle in the coronal plane (B). a=corpus callosum length, b=corpus callosum-fastigium distance, c=transcerebellar diameter, d=insular cortex height, e=cingulate sulcus depth and f=interopercular opening.
Cranial ultrasound linear measures of brain growth (A and B) and maturation (C). Images taken through the anterior fontanelle in the midsagittal plane (A) and coronal plane at the level of the foramina of Monro (C) and through the mastoid fontanelle in the coronal plane (B). a=corpus callosum length, b=corpus callosum-fastigium distance, c=transcerebellar diameter, d=insular cortex height, e=cingulate sulcus depth and f=interopercular opening.