
Emergency Medicine 6
Session: Emergency Medicine 6
Kaileen Jafari, MD
Assistant Professor
University of Washington School of Medicine
Seattle Children's Hospital
Seattle, Washington, United States
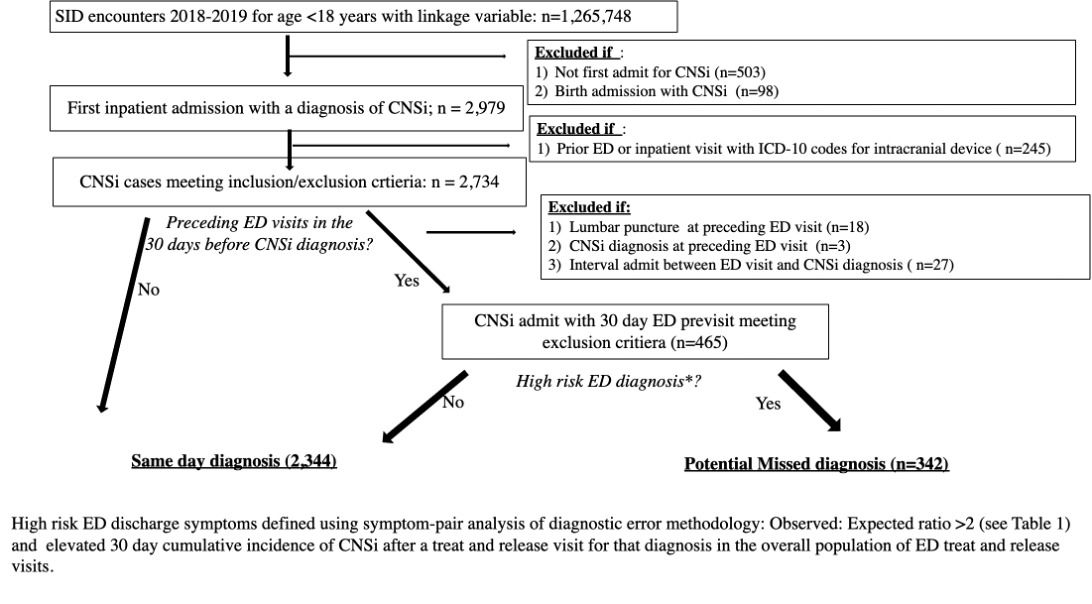
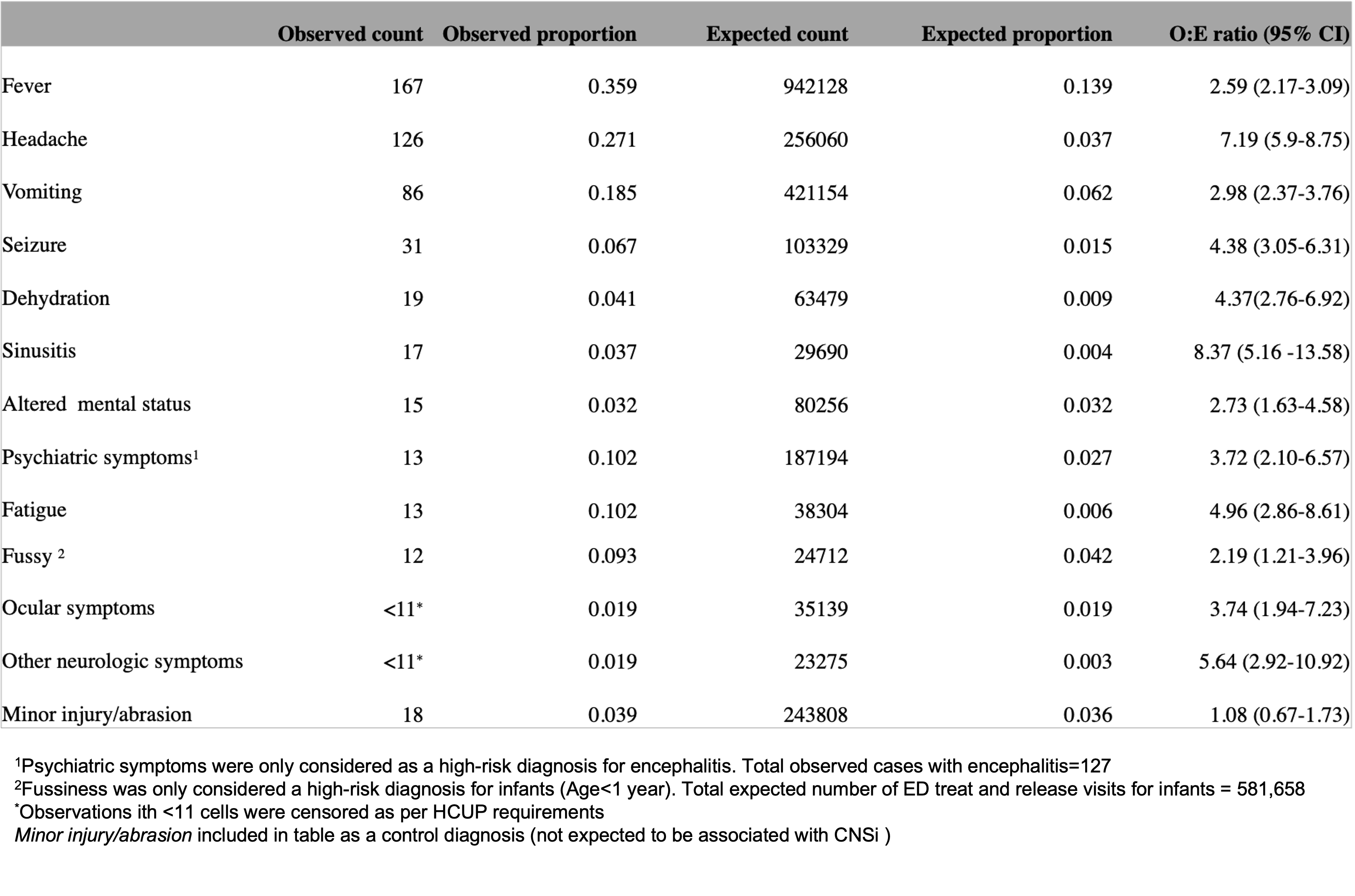 Observed:Expected ratio is the ratio of observed proportion (proportion of diagnosis in ED visits preceding CNSi diagnosis) to expected proportion (proportion of that diagnosis in overall population of ED treat and release visits in the dataset).
Observed:Expected ratio is the ratio of observed proportion (proportion of diagnosis in ED visits preceding CNSi diagnosis) to expected proportion (proportion of that diagnosis in overall population of ED treat and release visits in the dataset). .png) A) Bacterial CNSi includes bacterial meningitis and craniospinal abscess and B) Viral or Other CNSi includes viral or other (fungal, atypical bacterial or unspecified) meningitis or encephalitis
A) Bacterial CNSi includes bacterial meningitis and craniospinal abscess and B) Viral or Other CNSi includes viral or other (fungal, atypical bacterial or unspecified) meningitis or encephalitis