
Neonatal General 1: Respiratory, BPD
Session: Neonatal General 1: Respiratory, BPD
 photo")
Victoria M. Scarpelli, MD MPH (she/her/hers)
Fellow, Neonatal Perinatal Medicine
Cohen Children's Medical Center
Mineola, New York, United States
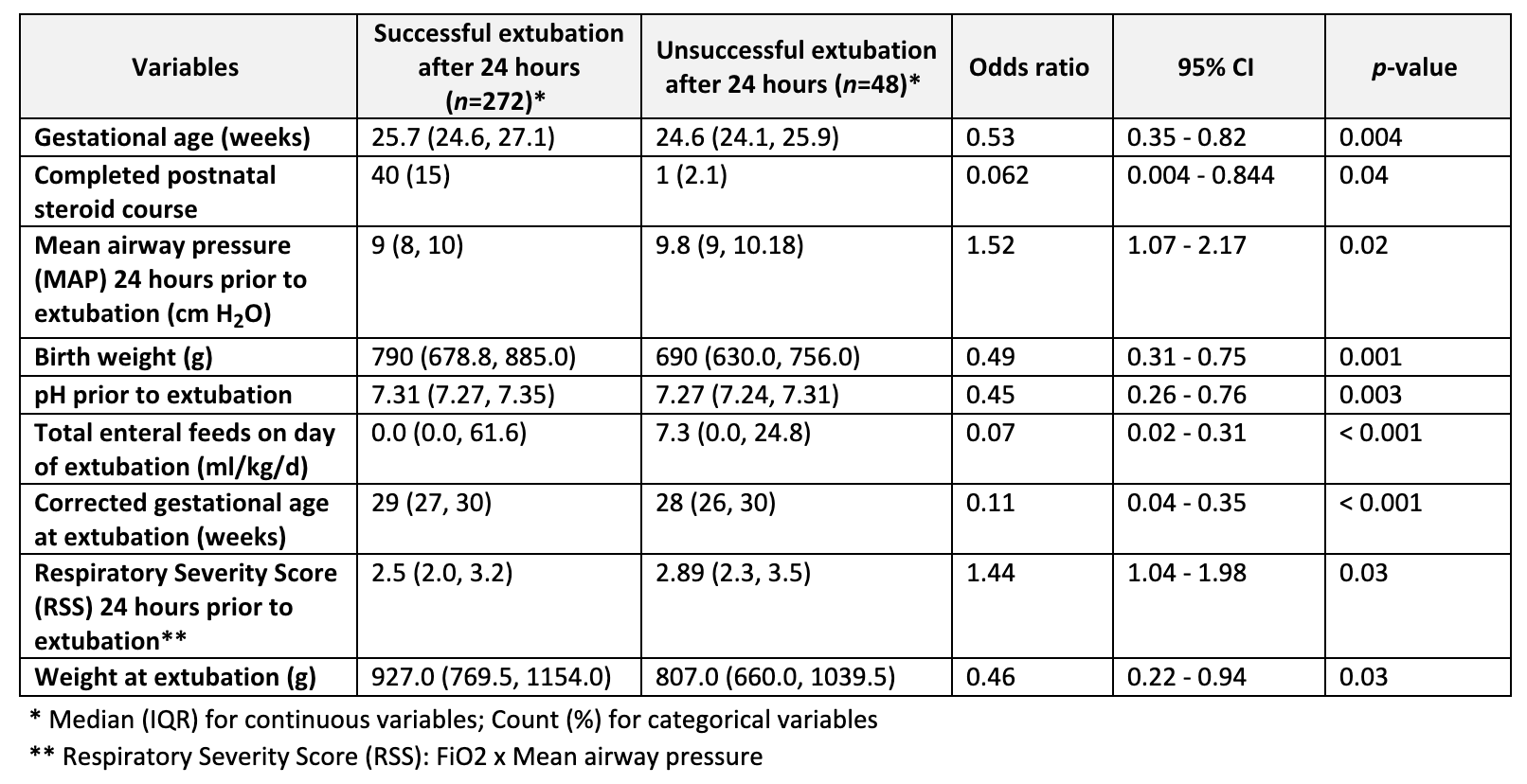 Nine variables were statistically significant as standalone predictors of extubation success in a mixed-effects logistic regression and were retained in the predictive model. Characteristics summarized with odds ratios and 95% confidence intervals.
Nine variables were statistically significant as standalone predictors of extubation success in a mixed-effects logistic regression and were retained in the predictive model. Characteristics summarized with odds ratios and 95% confidence intervals.