
Neonatal General 4: Novel Technology and Therapies
Session: Neonatal General 4: Novel Technology and Therapies

Eva Senechal, PhD
PhD. Candidate
McGill University Faculty of Medicine and Health Sciences
Montreal, Quebec, Canada
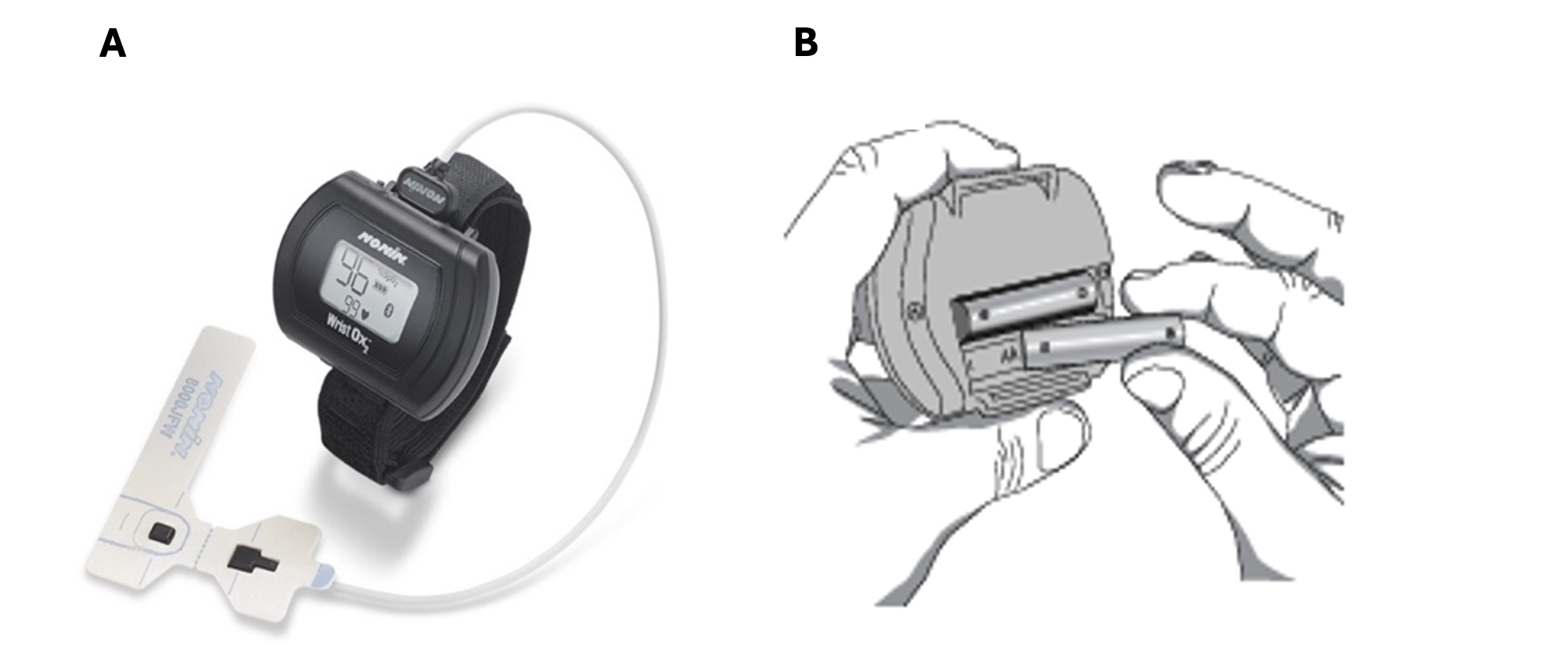 Legend: Figure A - Nonin WristOx2™ 3150 with 600CN attachment and Figure B - back of the device where AAA batteries to power the device are placed.
Legend: Figure A - Nonin WristOx2™ 3150 with 600CN attachment and Figure B - back of the device where AAA batteries to power the device are placed.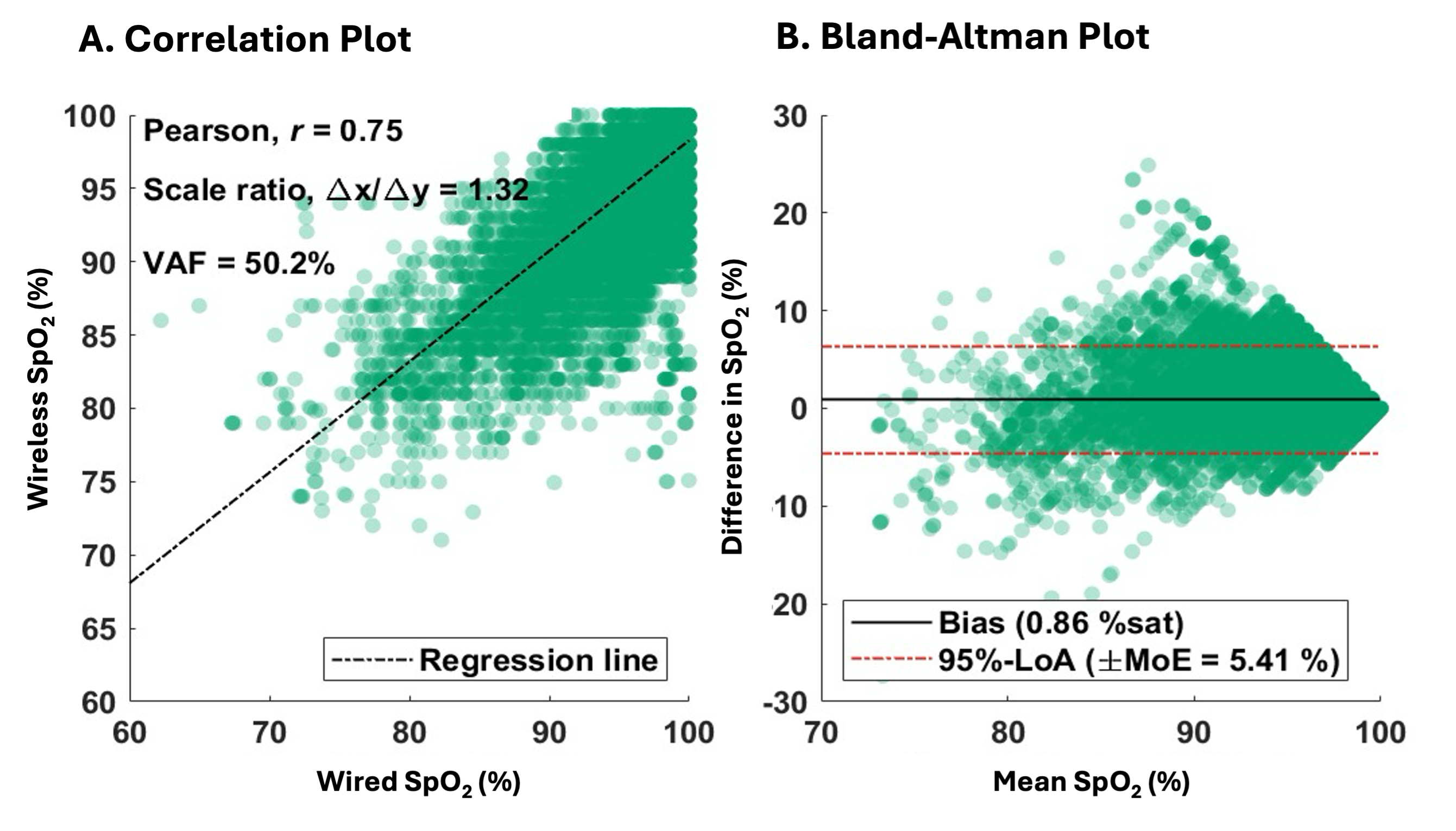 Legend: Panel A - linear regression of one patient with the pearson correlation coefficient, scale ration (slope), and variance accounted for (vaf). Panel B - Bland Altman analysis on the same patient with the bias, 95% limits of agreement (LoA) and margin of error (MoE).
Legend: Panel A - linear regression of one patient with the pearson correlation coefficient, scale ration (slope), and variance accounted for (vaf). Panel B - Bland Altman analysis on the same patient with the bias, 95% limits of agreement (LoA) and margin of error (MoE). 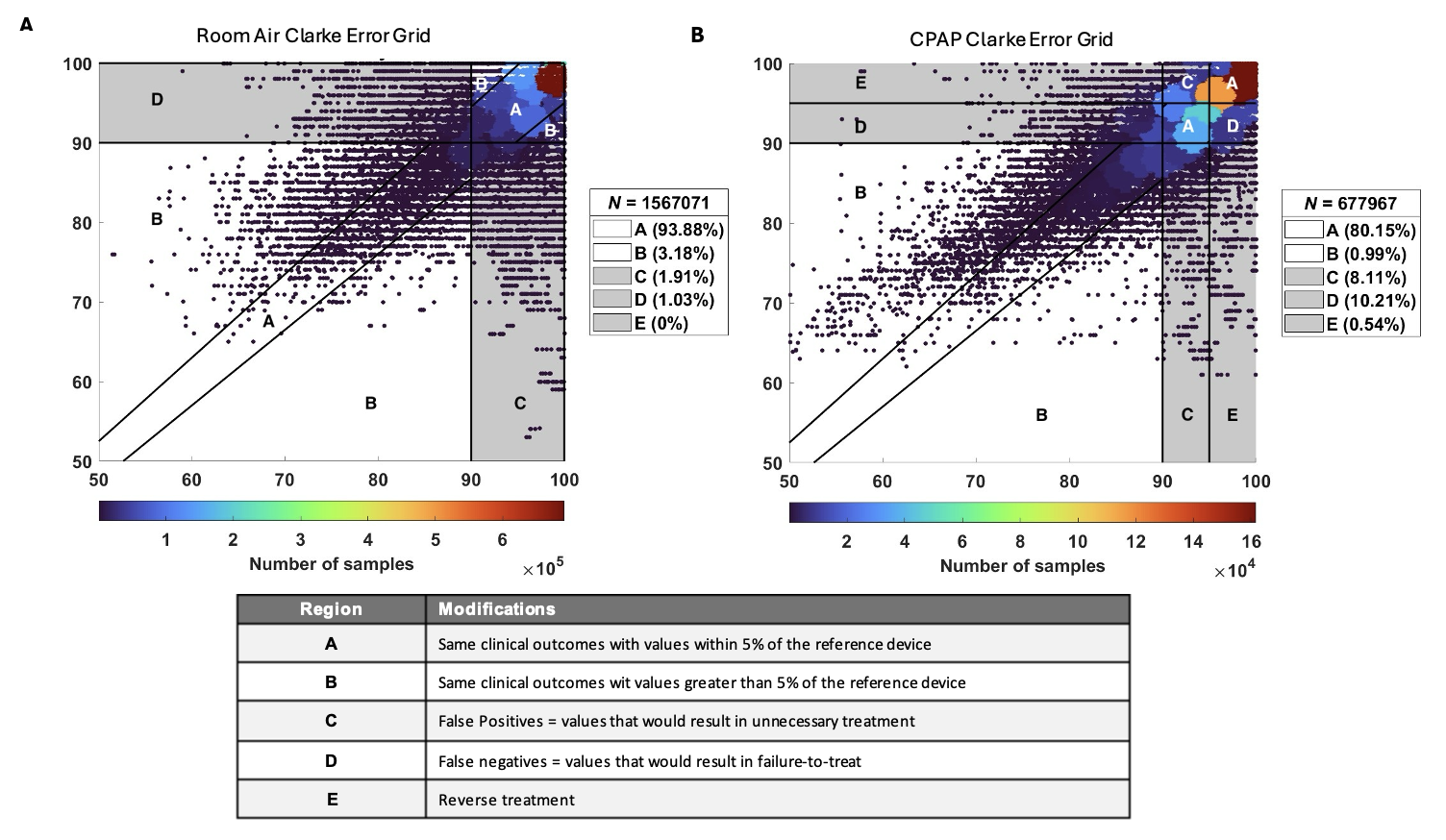 Legend: Panel A - Clarke Error Grid for patients on room air (RA, n=20). Panel B - Clarke Error Grid for patients on continuous positive airway pressure (CPAP, n=6). Any SpO2 value <90% was consider hypoxia and values >95% where considered hyperoxia. The percentage of data points assigned to each region is provided on the box at the right corner. Region definitions are provided in table below the figures.
Legend: Panel A - Clarke Error Grid for patients on room air (RA, n=20). Panel B - Clarke Error Grid for patients on continuous positive airway pressure (CPAP, n=6). Any SpO2 value <90% was consider hypoxia and values >95% where considered hyperoxia. The percentage of data points assigned to each region is provided on the box at the right corner. Region definitions are provided in table below the figures. 