
Global Neonatal & Children's Health 1
Session: Global Neonatal & Children's Health 1
Chris A. Rees, MD, MPH
Assistant Professor
Emory University School of Medicine
Atlanta, Georgia, United States
.jpg) Forty-eight (32.0%) blood cultures grew E. coli, of which 35.4% were resistant to ceftriaxone and 4.2% resistant to meropenem. Thirty-nine (27.5%) blood cultures grew K. pneumoniae; of which 51.3% were resistant to ceftriaxone and 10.3% had intermediate resistance to meropenem.
Forty-eight (32.0%) blood cultures grew E. coli, of which 35.4% were resistant to ceftriaxone and 4.2% resistant to meropenem. Thirty-nine (27.5%) blood cultures grew K. pneumoniae; of which 51.3% were resistant to ceftriaxone and 10.3% had intermediate resistance to meropenem.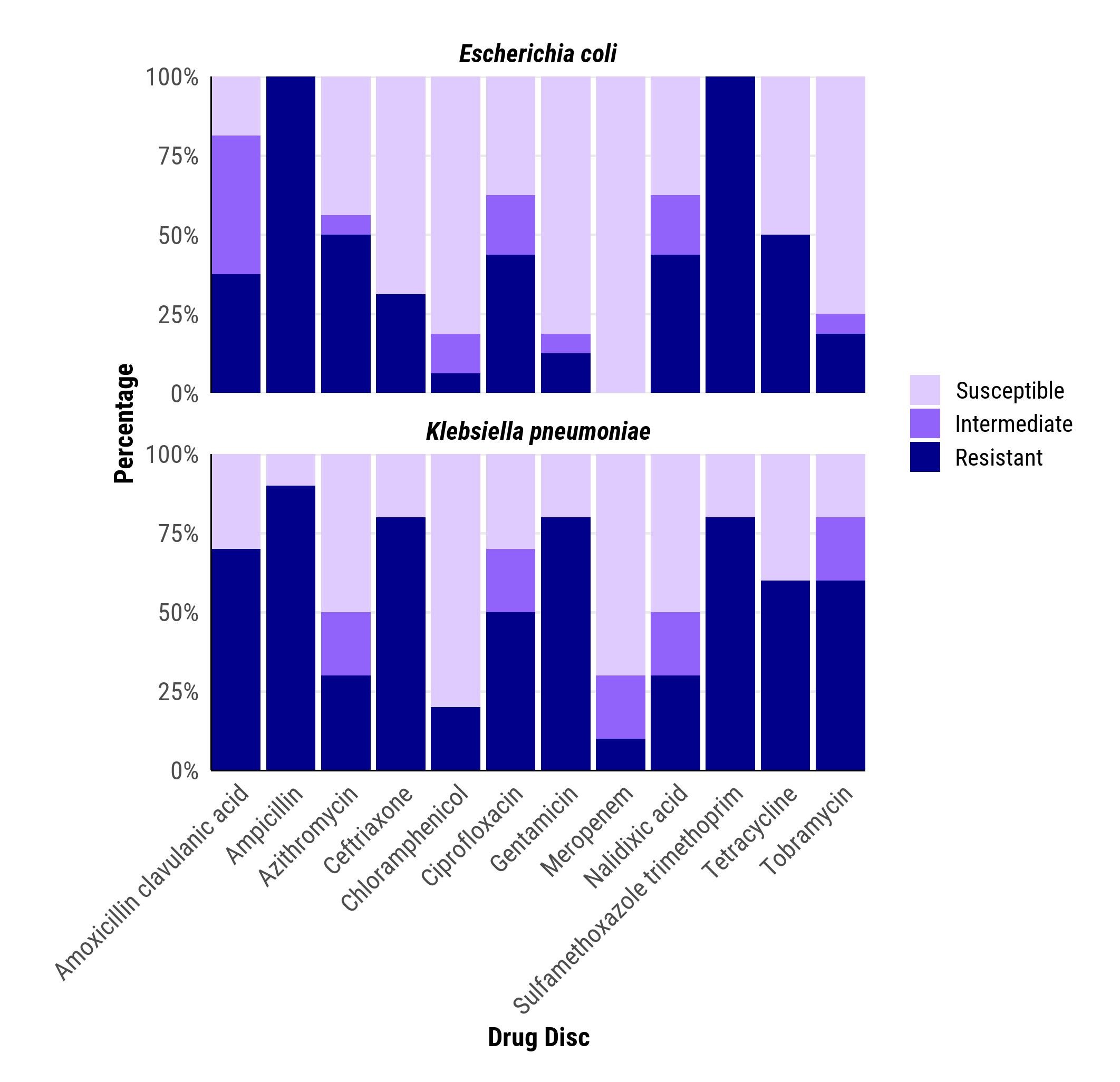 Sixteen (47.1%) of CSF cerebrospinal fluid isolates had E. coli, all of which were susceptible to meropenem, and 5 (31.2%) were resistant to ceftriaxone. Ten (29.4%) CSF cultures grew K. pneumoniae, of which 8 (80.0%) were resistant to ceftriaxone.
Sixteen (47.1%) of CSF cerebrospinal fluid isolates had E. coli, all of which were susceptible to meropenem, and 5 (31.2%) were resistant to ceftriaxone. Ten (29.4%) CSF cultures grew K. pneumoniae, of which 8 (80.0%) were resistant to ceftriaxone..jpg) Antimicrobial resistance to Amoxicillin Clavulanic acid and Ceftriaxone(commonly used drugs) was greatest among neonates and 1-59 month-old children.
Antimicrobial resistance to Amoxicillin Clavulanic acid and Ceftriaxone(commonly used drugs) was greatest among neonates and 1-59 month-old children.