
Neonatal Pulmonology - Clinical 2: BPD: Incidence, Treatment, Outcomes
Session: Neonatal Pulmonology - Clinical 2: BPD: Incidence, Treatment, Outcomes
Ryo Ogawa, N/A, MD,PhD (he/him/his)
Vice Director
Nagano Children's Hospital
Azumino, Nagano, Japan
.jpg) The most predominant SpO2 threshold was 95% (37%), with all facilities using values between 90% and 95%. Only 35% of the facilities had established standards for the duration and frequency of sub-threshold SpO2 levels.
The most predominant SpO2 threshold was 95% (37%), with all facilities using values between 90% and 95%. Only 35% of the facilities had established standards for the duration and frequency of sub-threshold SpO2 levels. 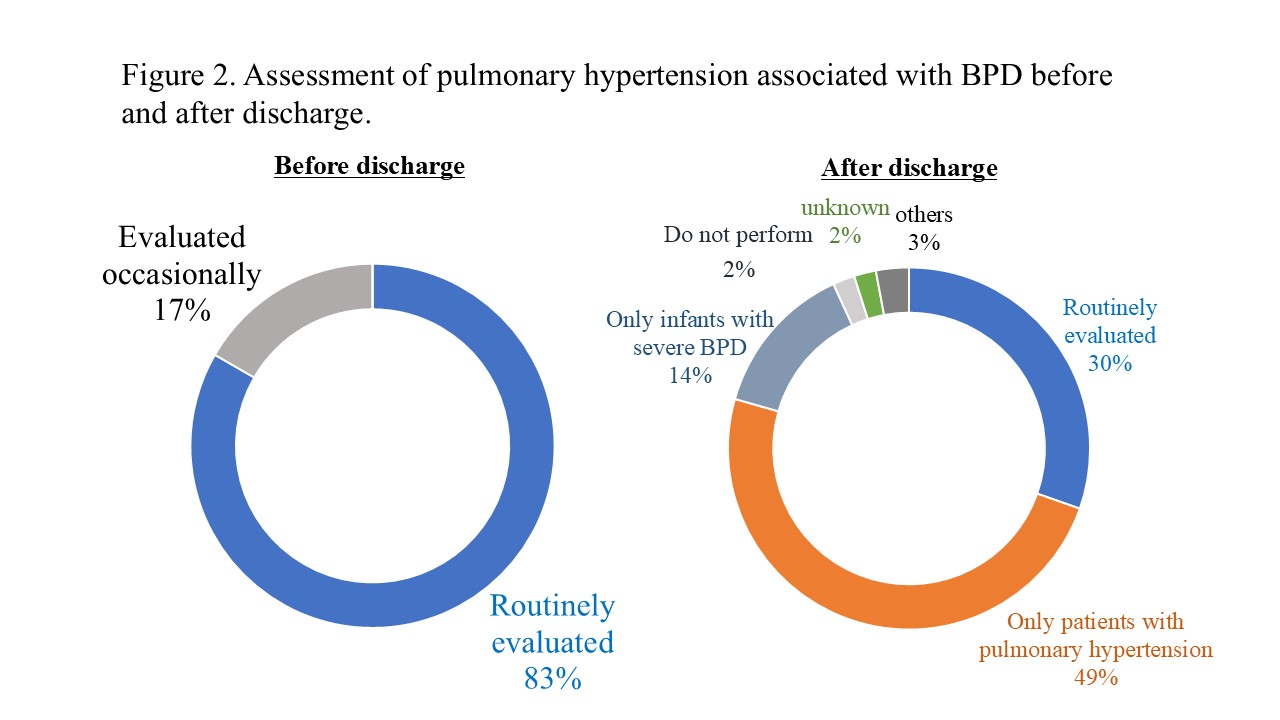 Pulmonary hypertension (PH) assessment was routinely performed in 83% of the facilities. However, only 30% of the facilities consistently conducted PH assessments after discharge.
Pulmonary hypertension (PH) assessment was routinely performed in 83% of the facilities. However, only 30% of the facilities consistently conducted PH assessments after discharge.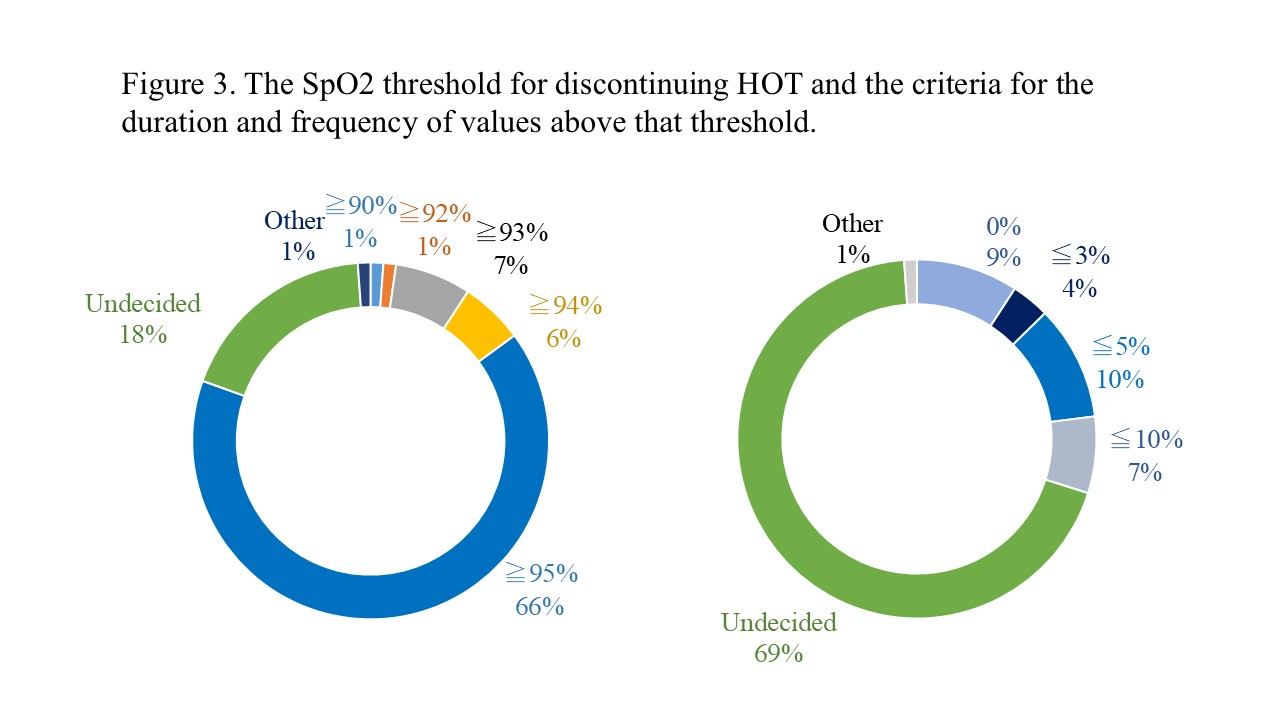 Of the facilities, 66% used a SpO2 threshold of ≥95% for discontinuation, but 69% lacked criteria for the duration and frequency of values below this threshold.
Of the facilities, 66% used a SpO2 threshold of ≥95% for discontinuation, but 69% lacked criteria for the duration and frequency of values below this threshold. 