
Emergency Medicine 5
Session: Emergency Medicine 5
 photo")
Vincent Patrick Uy, MD (he/him/his)
Assistant Professor
Weill Cornell Medicine
New York, New York, United States
.png) Table 1: Demographic Information
Table 1: Demographic Information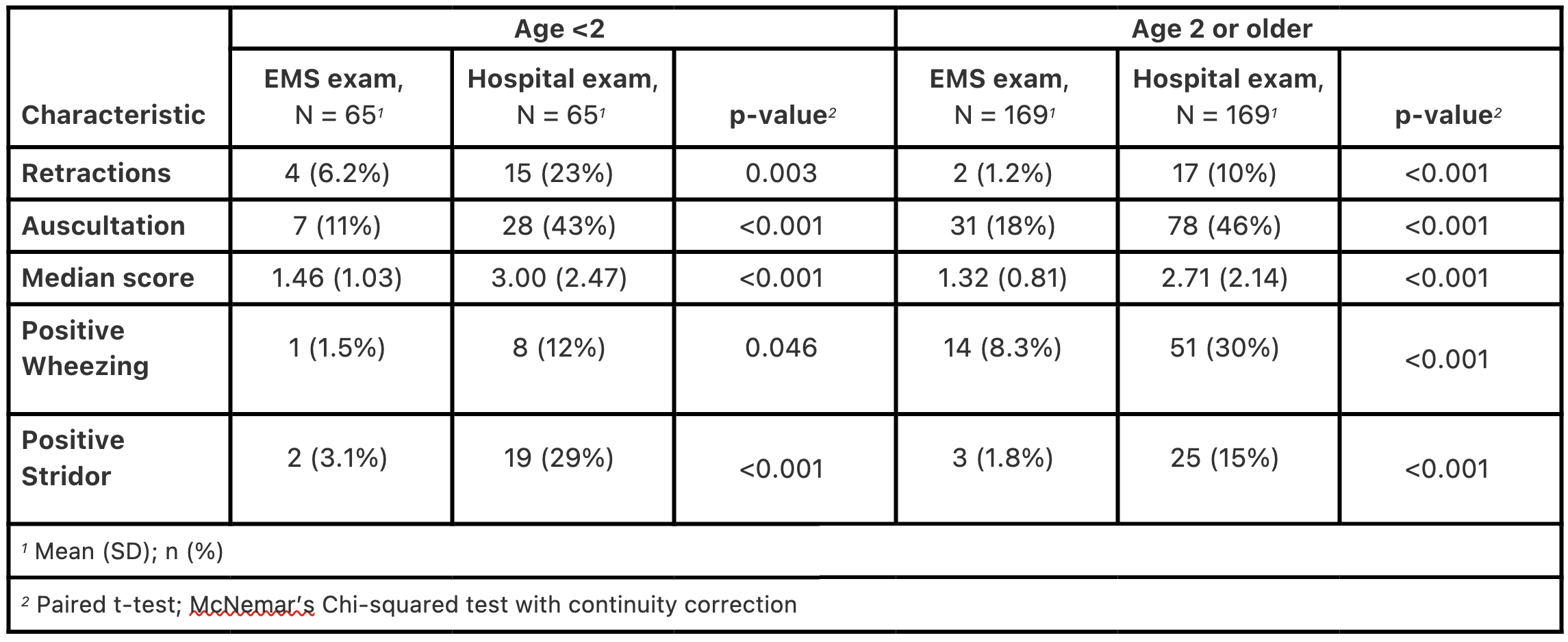 Table 2: Cross-sectional results Table 1: Demographic InformationTable 2: Cross-sectional results
Table 2: Cross-sectional results Table 1: Demographic InformationTable 2: Cross-sectional results 