
Neonatal Nephrology/AKI 2
Session: Neonatal Nephrology/AKI 2
 photo")
Arwa Nada, MD., MSc. (she/her/hers)
Associate Professor
Loma Linda University Children's Hospital
Loma Linda, California, United States
.png) Table.1: Demographic Data & Dialysis Modalities
Table.1: Demographic Data & Dialysis Modalities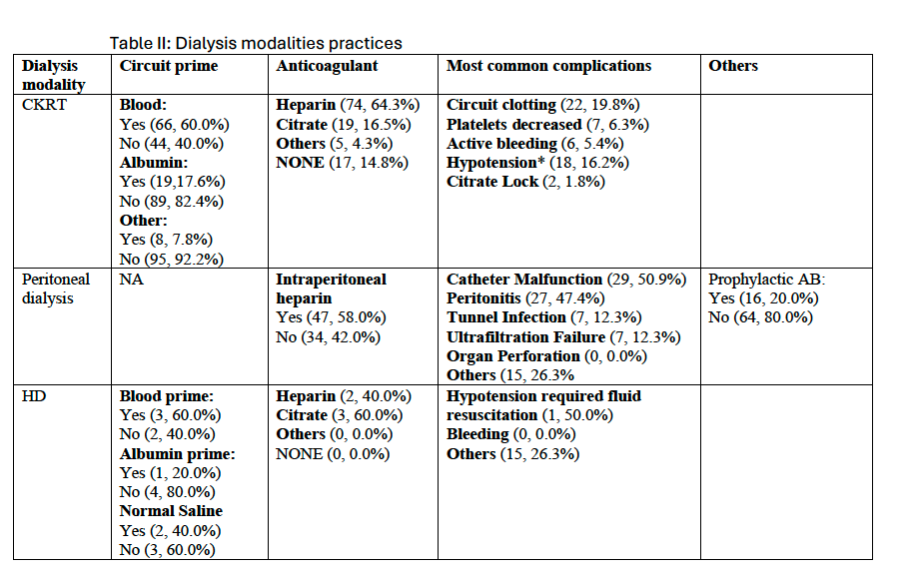 Table II: Dialysis modalities practices
Table II: Dialysis modalities practices