
Health Equity/Social Determinants of Health 2
Session: Health Equity/Social Determinants of Health 2
 photo")
Stephanie Diggs, MD, MSCI (she/her/hers)
Instructor
Washington University in St. Louis School of Medicine
Saint Louis, Missouri, United States
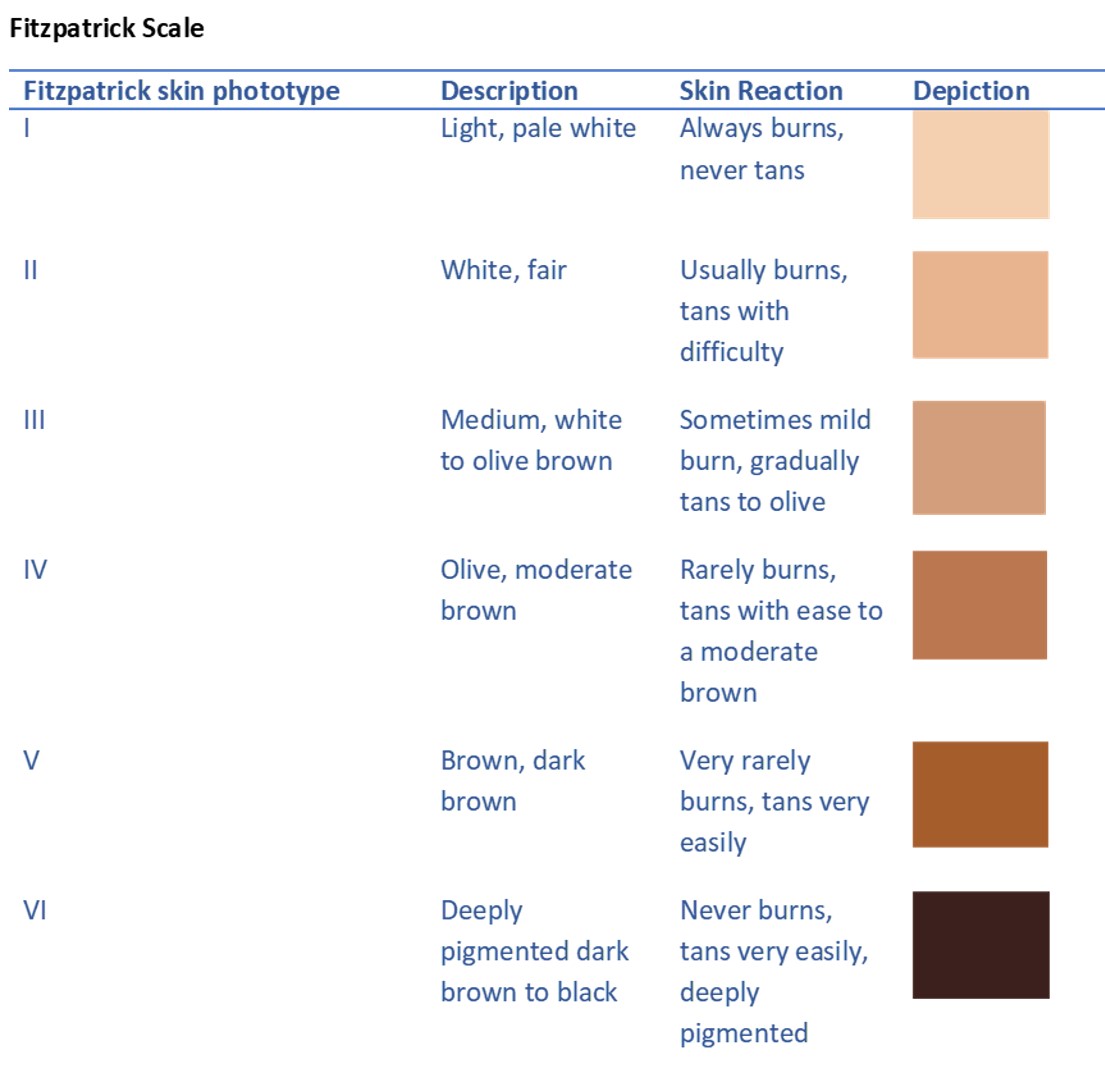 Figure 1. Fitzpatrick scale: A subjective scale outlining the associated skin appearance descriptions and reactions to sun exposure for each subgroup skin phototype I-VI.
Figure 1. Fitzpatrick scale: A subjective scale outlining the associated skin appearance descriptions and reactions to sun exposure for each subgroup skin phototype I-VI.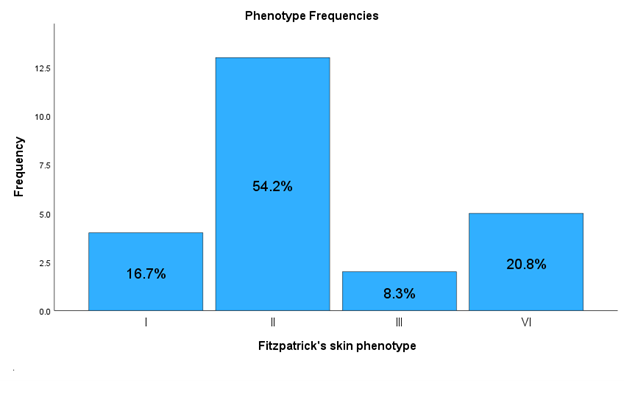 Figure 2. Fitzpatrick skin phenotype frequencies. Of note, no infants were categorized as having type IV or type V skin phenotypes.
Figure 2. Fitzpatrick skin phenotype frequencies. Of note, no infants were categorized as having type IV or type V skin phenotypes. .png) Figure 3. Distribution of melanin concentration for the Fitzpatrick skin phenotypes. Of note, no infants were categorized as having type IV or type V skin phenotypes. Figure 1. Fitzpatrick scale: A subjective scale outlining the associated skin appearance descriptions and reactions to sun exposure for each subgroup skin phototype I-VI.Figure 2. Fitzpatrick skin phenotype frequencies. Of note, no infants were categorized as having type IV or type V skin phenotypes. Figure 3. Distribution of melanin concentration for the Fitzpatrick skin phenotypes. Of note, no infants were categorized as having type IV or type V skin phenotypes.
Figure 3. Distribution of melanin concentration for the Fitzpatrick skin phenotypes. Of note, no infants were categorized as having type IV or type V skin phenotypes. Figure 1. Fitzpatrick scale: A subjective scale outlining the associated skin appearance descriptions and reactions to sun exposure for each subgroup skin phototype I-VI.Figure 2. Fitzpatrick skin phenotype frequencies. Of note, no infants were categorized as having type IV or type V skin phenotypes. Figure 3. Distribution of melanin concentration for the Fitzpatrick skin phenotypes. Of note, no infants were categorized as having type IV or type V skin phenotypes. 