
Neo-Perinatal Health Care Delivery: Epidemiology/Health Services Research 3
Session: Neo-Perinatal Health Care Delivery: Epidemiology/Health Services Research 3
Matthew Loop, PhD
Assistant Professor
Auburn University
Auburn, Alabama, United States
.png) Estimated county-level infant mortality rates per 1,000 births, as a function of county-level mortality rates with opioid poisoning as a contributing cause of death per 100,000 females aged 15 - 44 years. Associations are presented by mean county-level Area Deprivation Index (ADI) quartile.
Estimated county-level infant mortality rates per 1,000 births, as a function of county-level mortality rates with opioid poisoning as a contributing cause of death per 100,000 females aged 15 - 44 years. Associations are presented by mean county-level Area Deprivation Index (ADI) quartile.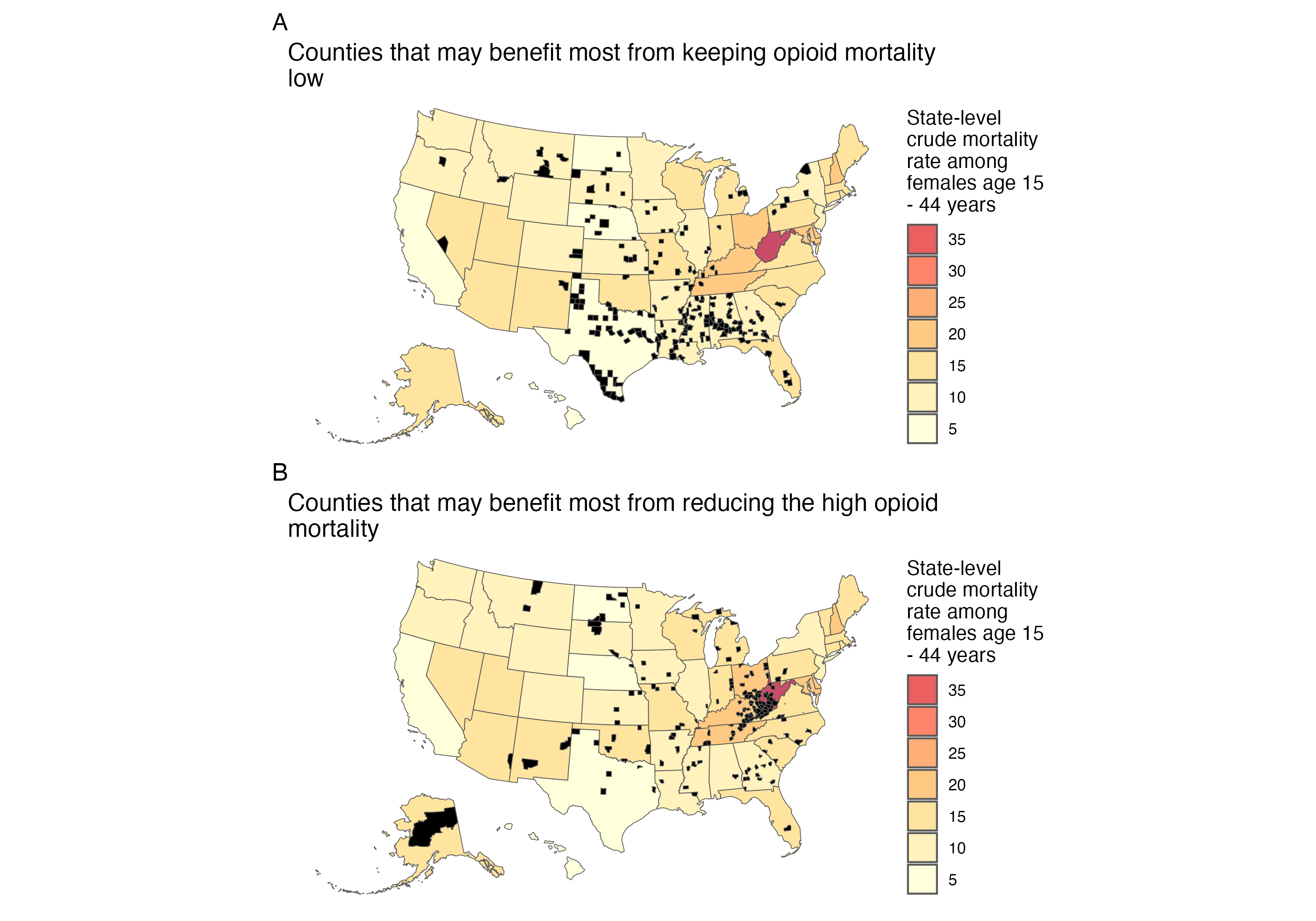 Where could we intervene? (A) Prophylaxis Counties in black are highly deprived (area deprivation index >= 75) but currently have < 5 opioid deaths per 100,000 females aged 15 - 44 years. Higher infant mortality rises the fastest with higher opioid mortality in these counties with high ADI (see Figure 1), so keeping the opioid epidemic from increasing in these counties may prevent the most infant deaths. These counties are concentrated in the Deep South and Midwest. (B) Treatment Counties in black are highly deprived (area deprivation index >= 75) but currently have > 20 opioid deaths per 100,000 females aged 15 - 44 years. Higher infant mortality rises the fastest with higher opioid mortality in these counties with high ADI (see Figure 1), so reducing the opioid epidemic from currently high levels in these counties may prevent the most infant deaths. These counties are concentrated in Appalachia.
Where could we intervene? (A) Prophylaxis Counties in black are highly deprived (area deprivation index >= 75) but currently have < 5 opioid deaths per 100,000 females aged 15 - 44 years. Higher infant mortality rises the fastest with higher opioid mortality in these counties with high ADI (see Figure 1), so keeping the opioid epidemic from increasing in these counties may prevent the most infant deaths. These counties are concentrated in the Deep South and Midwest. (B) Treatment Counties in black are highly deprived (area deprivation index >= 75) but currently have > 20 opioid deaths per 100,000 females aged 15 - 44 years. Higher infant mortality rises the fastest with higher opioid mortality in these counties with high ADI (see Figure 1), so reducing the opioid epidemic from currently high levels in these counties may prevent the most infant deaths. These counties are concentrated in Appalachia.