Infectious Diseases 4: Improving antibiotic use
Session: Infectious Diseases 4: Improving antibiotic use

Joel Rose-Kamprath, MS, MD
Resident Physician
Dell Children's Medical Center of Central Texas
Austin, Texas, United States
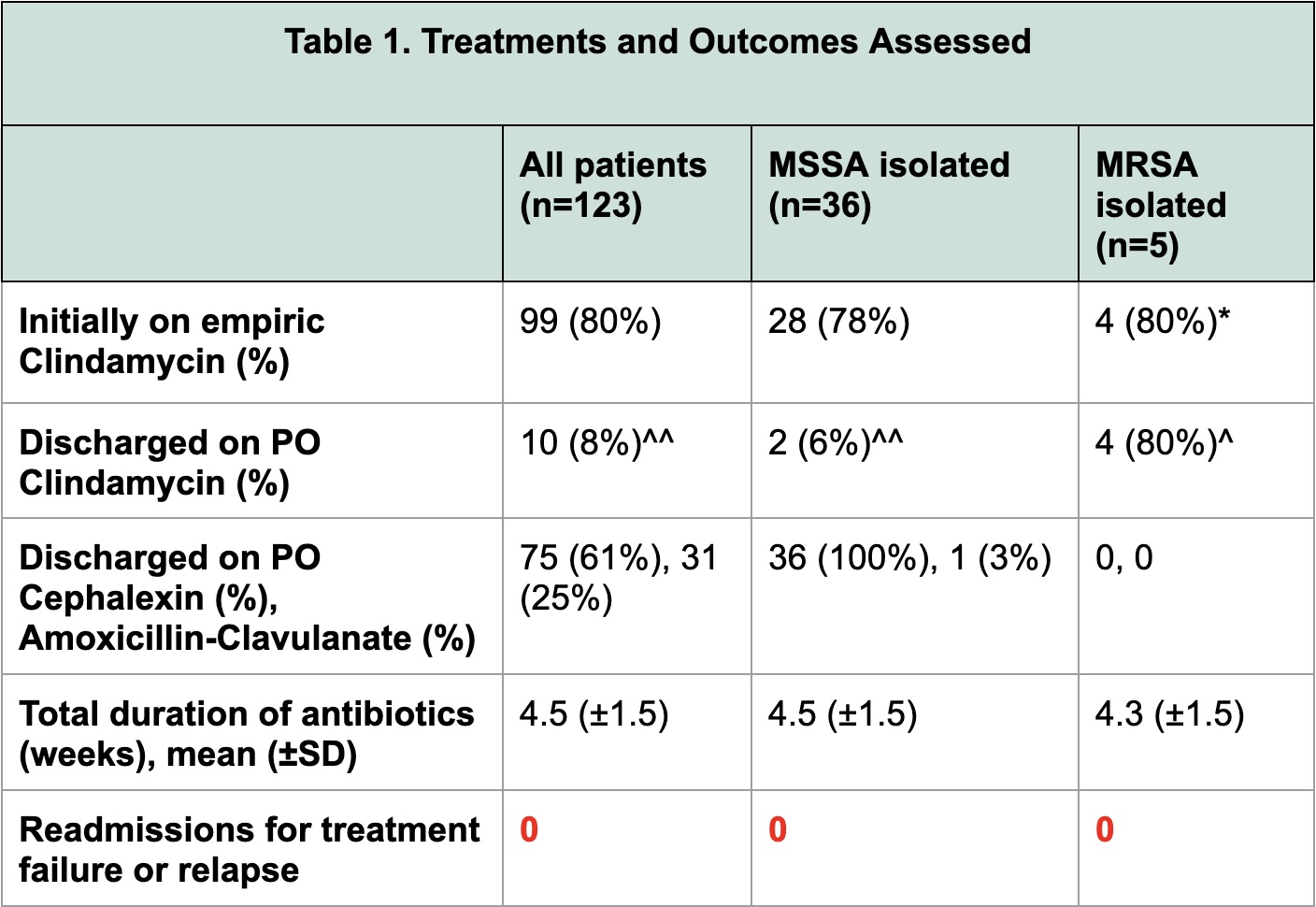 *One patient was initially on Vancomycin
*One patient was initially on Vancomycin