
Neo-Perinatal Health Care Delivery: Epidemiology/Health Services Research 2
Session: Neo-Perinatal Health Care Delivery: Epidemiology/Health Services Research 2
Brian King, MD (he/him/his)
Assistant Professor of Pediatrics
Harvard Medical School
Boston, Massachusetts, United States
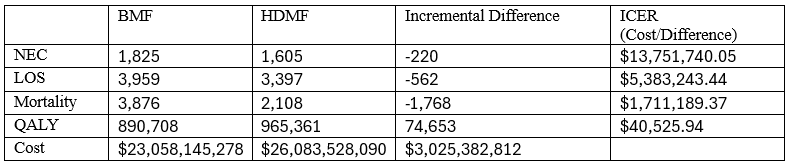 Base case analysis used the point estimates for risk ratios (RR) from a meta-analysis of two published randomized trials (Optimom and N-Forte), which were as follows: NEC 0.89 (95% CI 0.41 to 1.97), Late-onset sepsis 0.86 (95% CI 0.41 to 1.77) and Mortality 0.57 (95% CI 0.27 to 1.22).
Base case analysis used the point estimates for risk ratios (RR) from a meta-analysis of two published randomized trials (Optimom and N-Forte), which were as follows: NEC 0.89 (95% CI 0.41 to 1.97), Late-onset sepsis 0.86 (95% CI 0.41 to 1.77) and Mortality 0.57 (95% CI 0.27 to 1.22).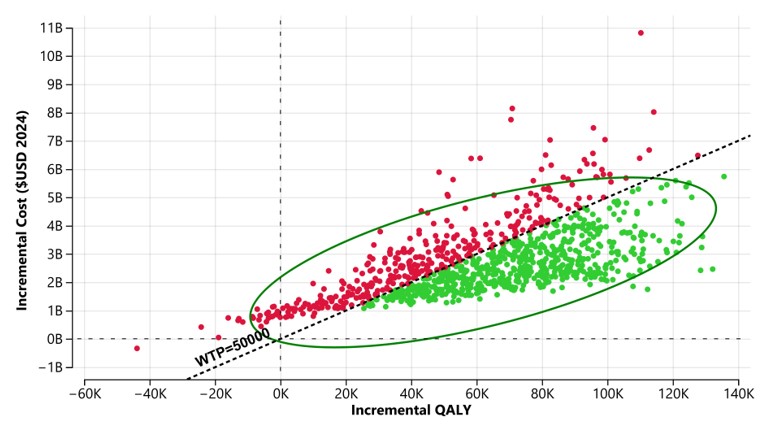 Probabilistic sensitivity analysis over 10,000 iterations which vary the effect estimates for reduction in NEC, LOS and mortality from HDMF across the 95% confidence interval from a meta-analysis of two randomized controlled trials. Green dots indicate iterations that were cost-effective with a willingness-to-pay threshold of 50,000 per QALY. Ellipses represents 95% of the iterations.
Probabilistic sensitivity analysis over 10,000 iterations which vary the effect estimates for reduction in NEC, LOS and mortality from HDMF across the 95% confidence interval from a meta-analysis of two randomized controlled trials. Green dots indicate iterations that were cost-effective with a willingness-to-pay threshold of 50,000 per QALY. Ellipses represents 95% of the iterations.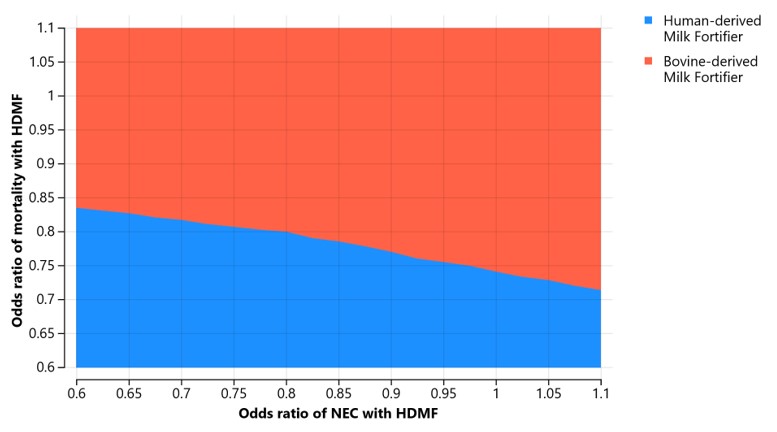 Color indicates which option is cost-effective using a WTP of $50,000 per QALY.
Color indicates which option is cost-effective using a WTP of $50,000 per QALY.