
Hospital Medicine 1: Quality Improvement
Session: Hospital Medicine 1: Quality Improvement
 Credit")
 photo")
Olivia Post, MD (she/her/hers)
Hospital Medicine Clinical Fellow
Cincinnati Children's Hospital Medical Center
Cincinnati, Ohio, United States
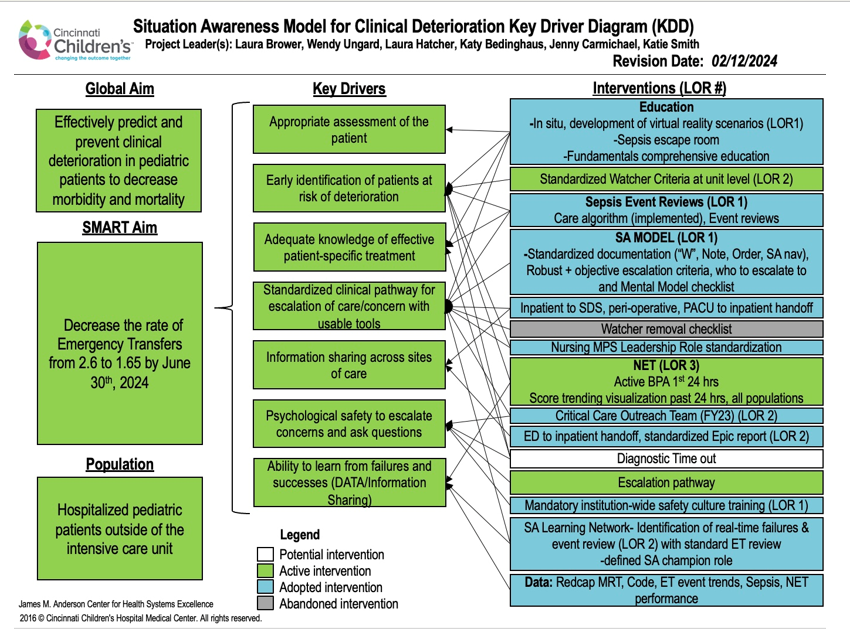 Key driver diagram for situation awareness model.
Key driver diagram for situation awareness model. 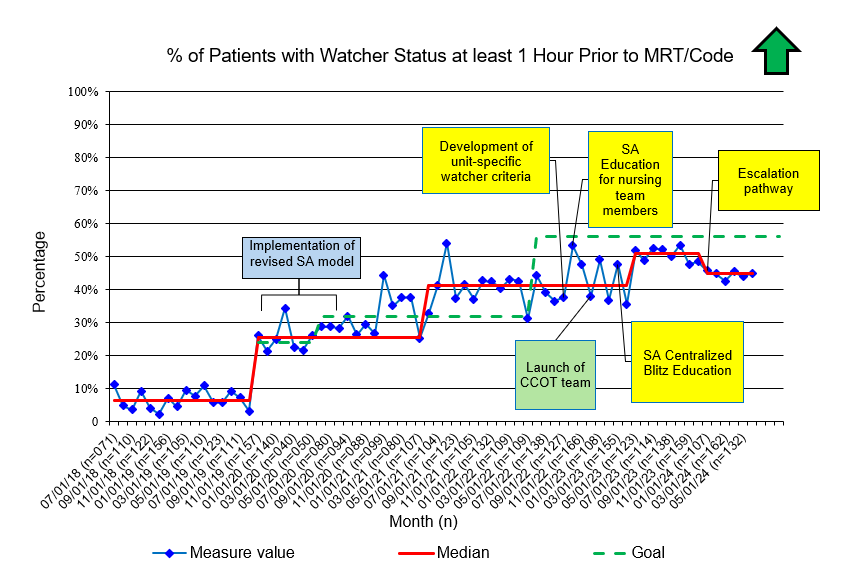 Run chart detailing percentage of patients with watcher status at least one hour prior to MRT or code. Interventions by situation awareness team are in yellow. Other institutional interventions which may have impacted the primary process measure are in green.
Run chart detailing percentage of patients with watcher status at least one hour prior to MRT or code. Interventions by situation awareness team are in yellow. Other institutional interventions which may have impacted the primary process measure are in green. 