
Neonatal Hemodynamics and Cardiovascular Medicine 2
Session: Neonatal Hemodynamics and Cardiovascular Medicine 2

Robert Joyce, MRCPI MB BCh BAO
Neonatal Specialist Registrar
Cork University Maternity Hospital
Dublin, Dublin, Ireland
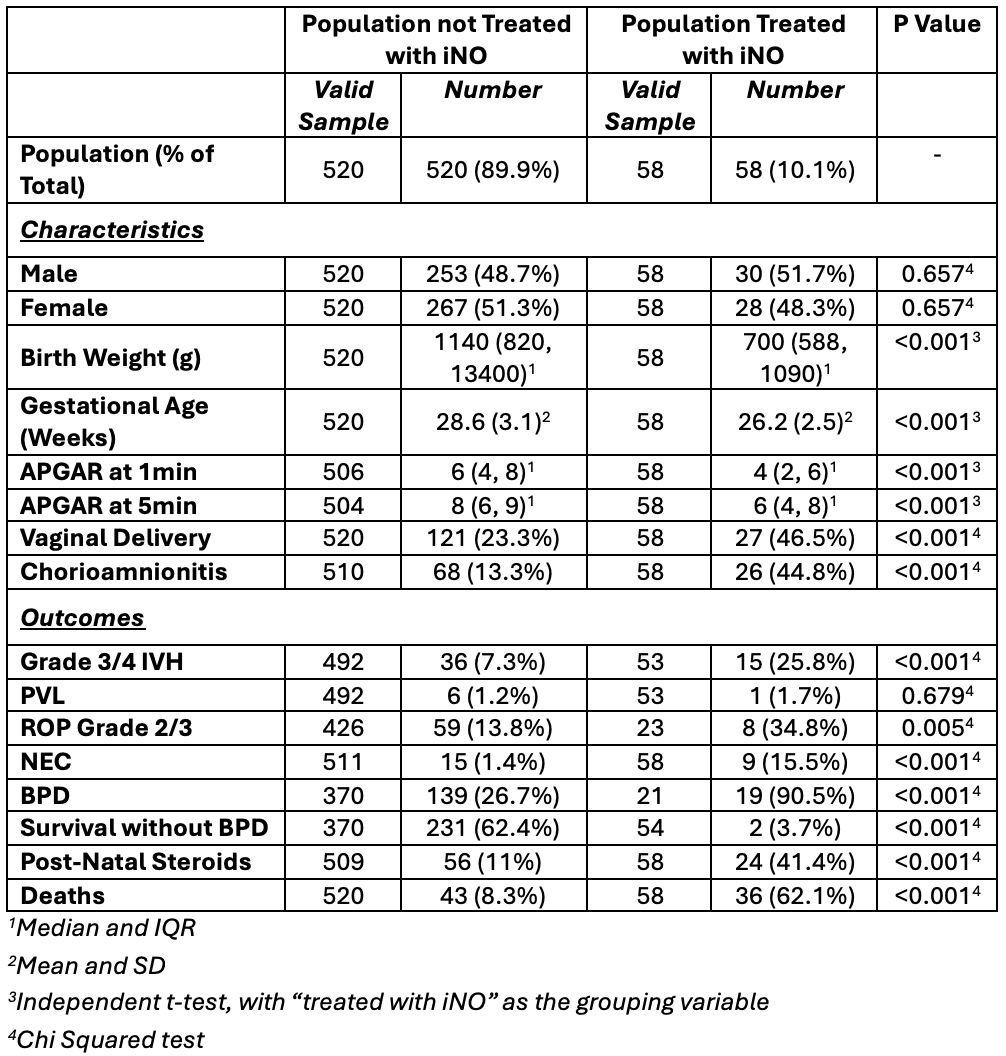 Population Comparisons
Population Comparisons.png) Pre and Post-iNO Initiation Respiratory Parameters
Pre and Post-iNO Initiation Respiratory Parameters.png) OSI Change by Characteristic
OSI Change by Characteristic