
Quality Improvement/Patient Safety 5
Session: Quality Improvement/Patient Safety 5
 Credit")
 photo")
Jesse A. Honig, MD (he/him/his)
Chief Resident
Cohen Children's Medical Center
New Hyde Park, New York, United States
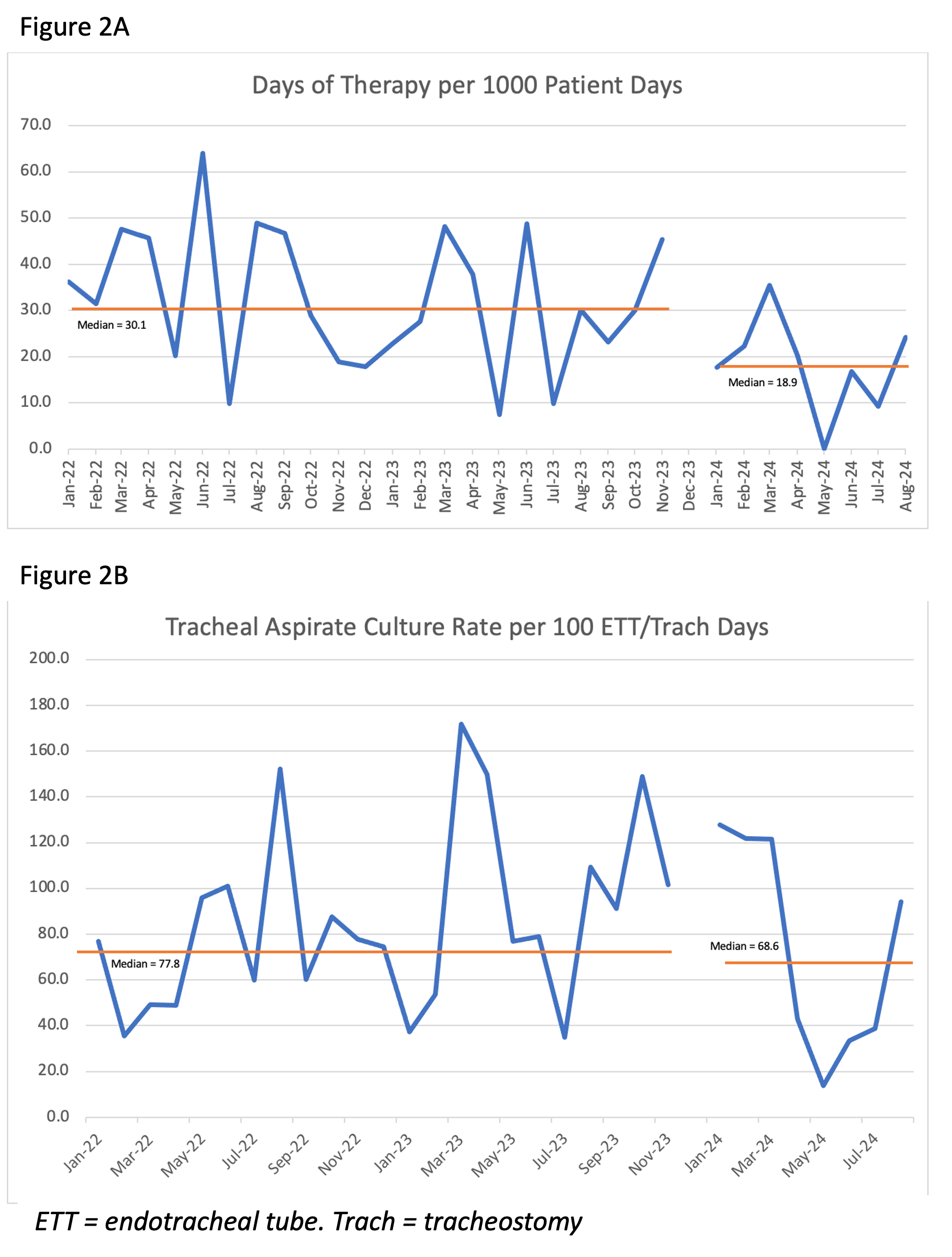 Figure 2A: Antibiotic days of therapy for ventilator associated tracheitis
Figure 2A: Antibiotic days of therapy for ventilator associated tracheitis