
Medical Education 3: Simulation
Session: Medical Education 3: Simulation

Sofia Grigoria Athanasopoulou, MD
Fellow in Pediatric Emergency Medicine
Yale School of Medicine
Yale School of Medicine
New Haven, Connecticut, United States
.png)
.png)
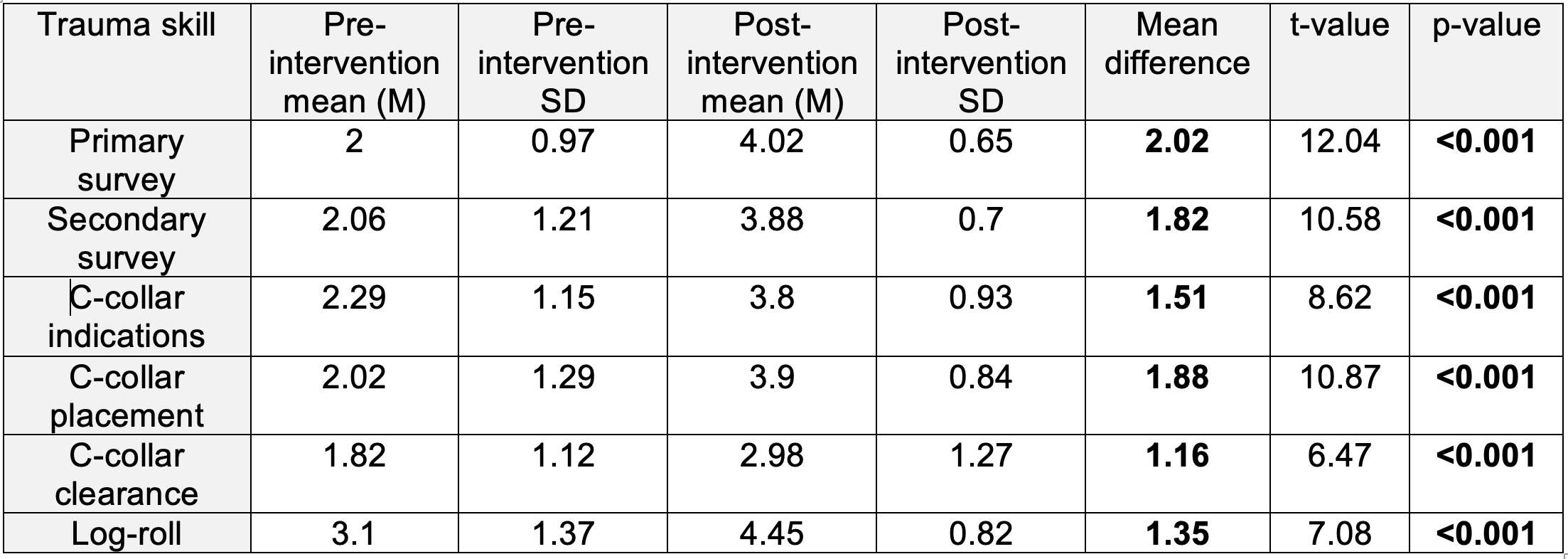 Range: 0 = Extremely Uncomfortable to 5 = Extremely Comfortable
Range: 0 = Extremely Uncomfortable to 5 = Extremely Comfortable