
Medical Education 3: Simulation
Session: Medical Education 3: Simulation
 photo")
Jonathan H. Pelletier, MD (he/him/his)
Assistant Professor
Akron Children’s Hospital
Akron, Ohio, United States
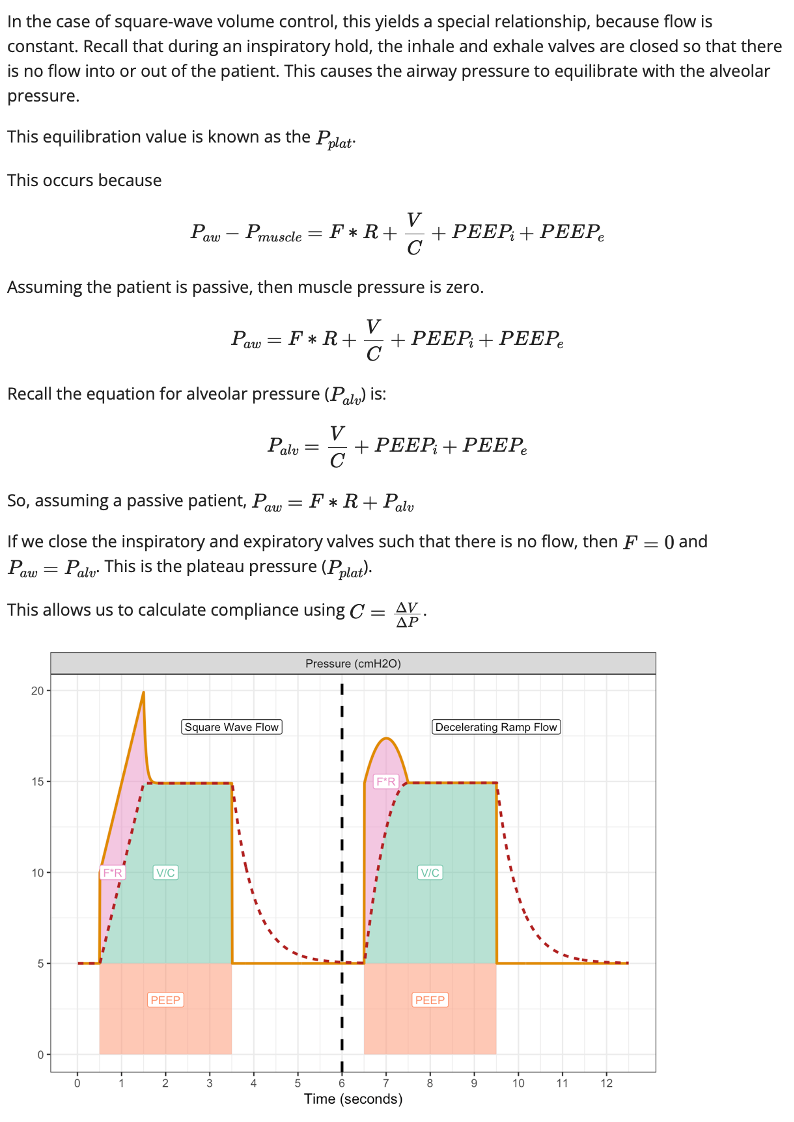 Sample reading materials from the "volume control" chapter of PrOVE.
Sample reading materials from the "volume control" chapter of PrOVE.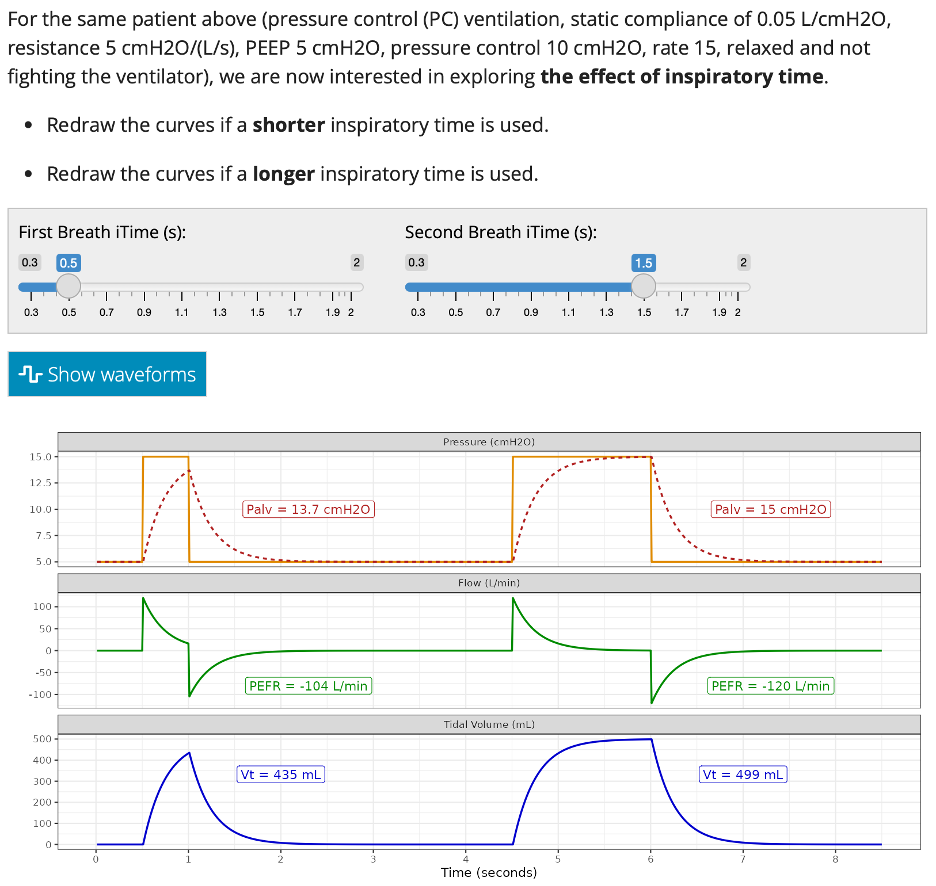 Sample interactive waveforms from the "pressure control" chapter of PrOVE.
Sample interactive waveforms from the "pressure control" chapter of PrOVE.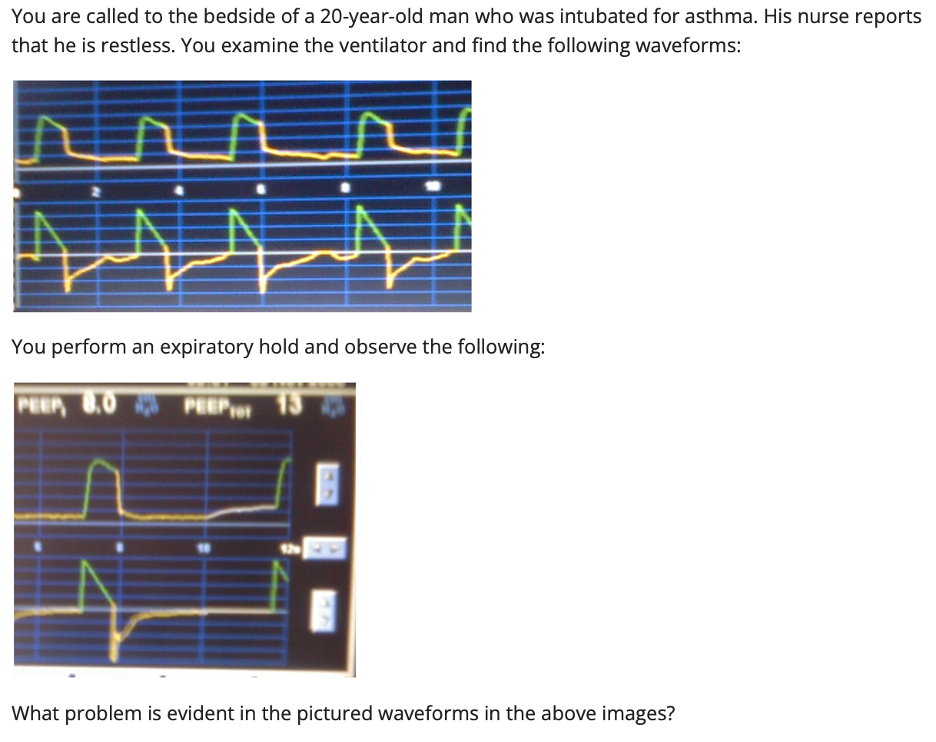 Sample patient case from the "expiratory waveforms" chapter of PrOVE.Sample reading materials from the "volume control" chapter of PrOVE.Sample interactive waveforms from the "pressure control" chapter of PrOVE.Sample patient case from the "expiratory waveforms" chapter of PrOVE.
Sample patient case from the "expiratory waveforms" chapter of PrOVE.Sample reading materials from the "volume control" chapter of PrOVE.Sample interactive waveforms from the "pressure control" chapter of PrOVE.Sample patient case from the "expiratory waveforms" chapter of PrOVE.