
Emergency Medicine 12
Session: Emergency Medicine 12
 photo")
Lyndsay J. Lee, Doctor of Medicine (she/her/hers)
Resident
Donald and Barbara Zucker School of Medicine at Hofstra/Northwell
Douglaston, New York, United States
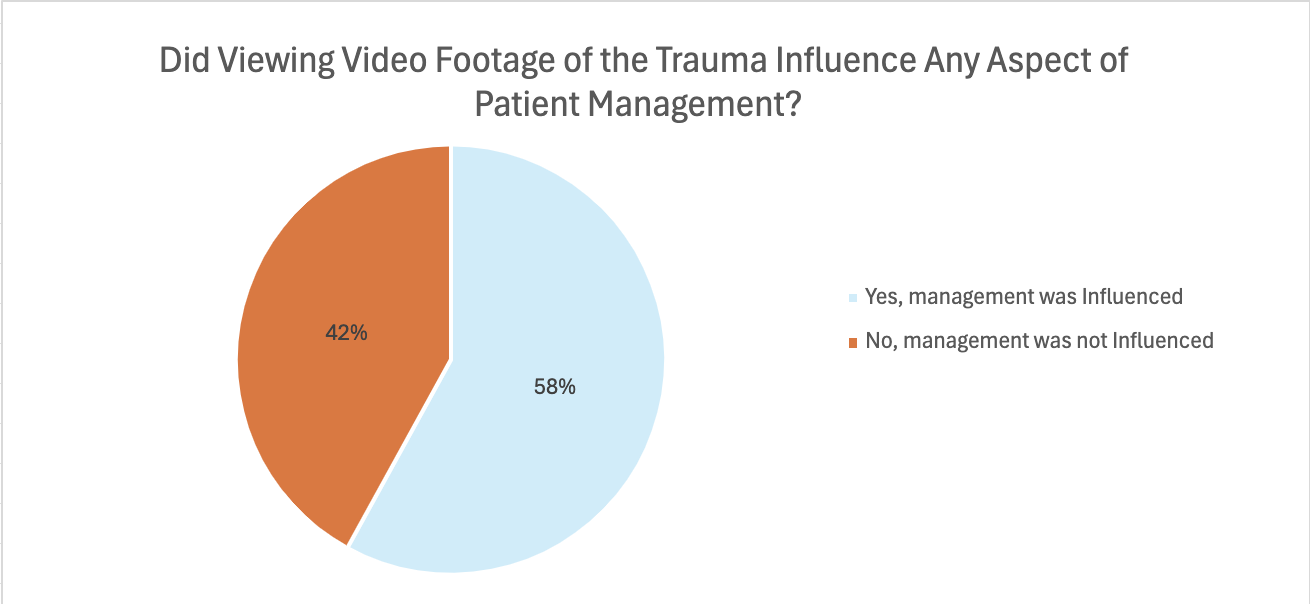 In 25 cases (58%), ED providers reported seeing the video influenced the management of their patient (total n= 43).
In 25 cases (58%), ED providers reported seeing the video influenced the management of their patient (total n= 43).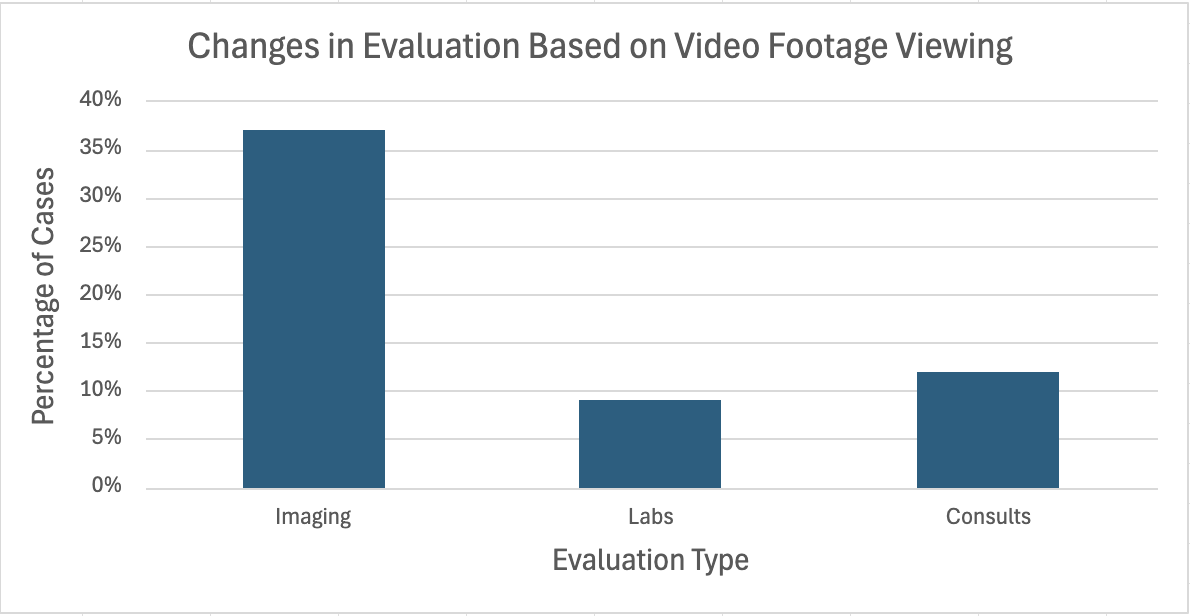 A review of the footage influenced providers’ decision regarding radiologic imaging in 16 cases (37%), lab studies in 4 cases (9%), and consults in 5 cases (12%) (total n= 25).
A review of the footage influenced providers’ decision regarding radiologic imaging in 16 cases (37%), lab studies in 4 cases (9%), and consults in 5 cases (12%) (total n= 25).