Children with Chronic Conditions 3
Session: Children with Chronic Conditions 3

Madhuradhar Chegondi, MD
Visiting Clinical Professor
University of Illinois College of Medicine
Peoria, Illinois, United States
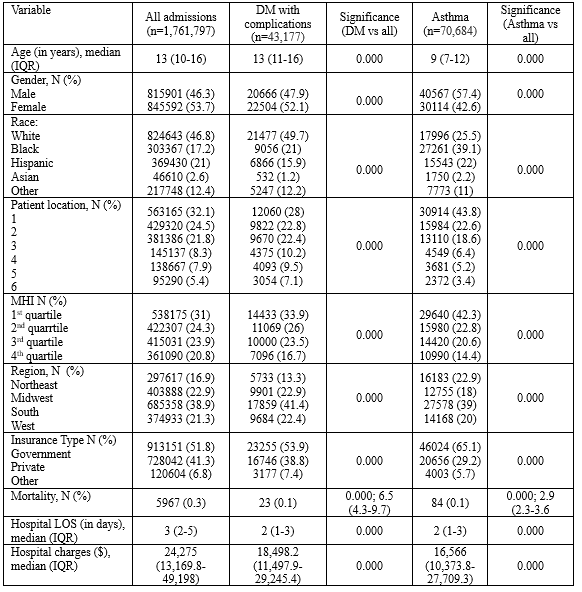 DM = diabetes; IQR= interquartile range; MHI = median household income; LOS= length of stay.
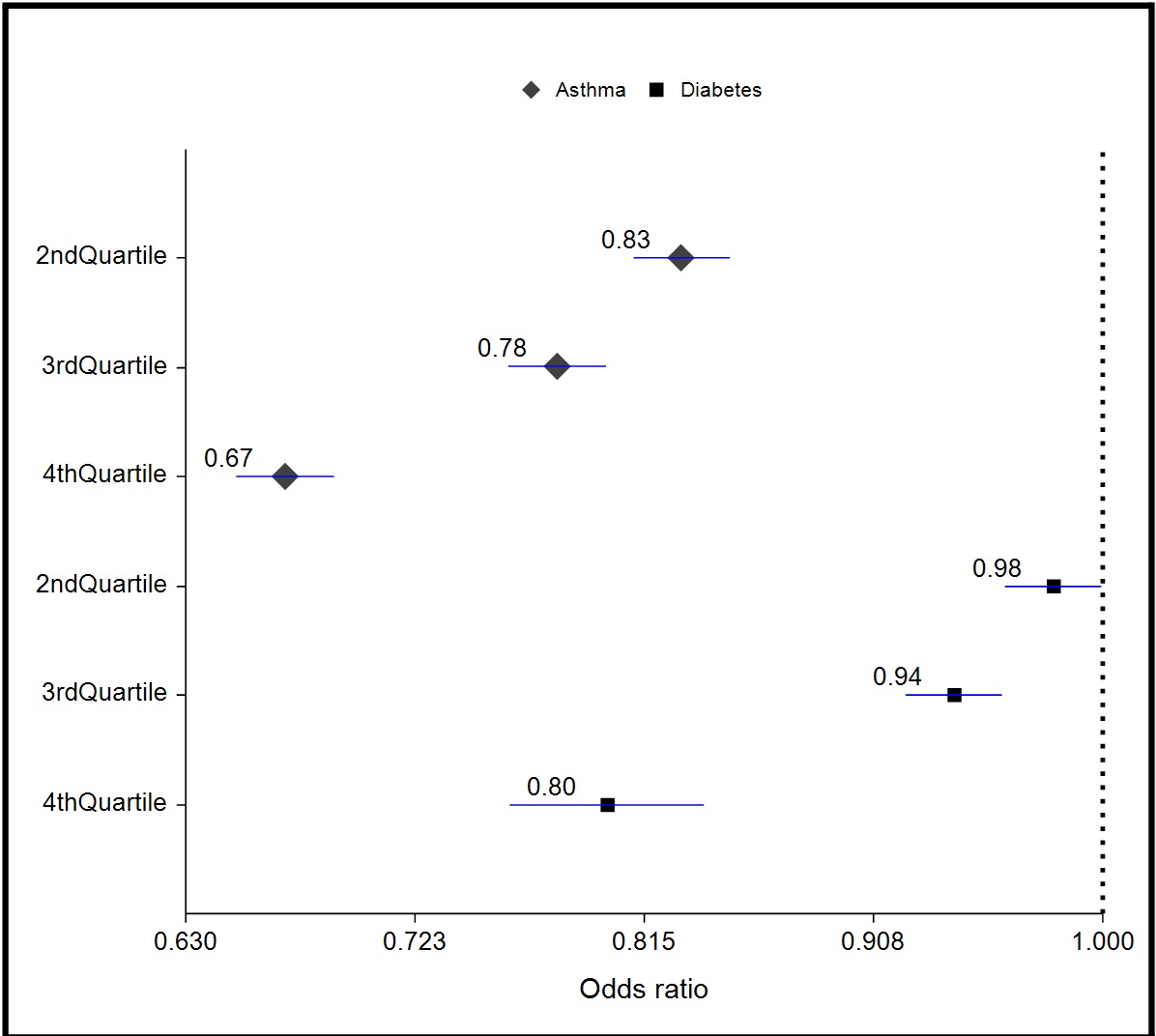
DM = diabetes; IQR= interquartile range; MHI = median household income; LOS= length of stay.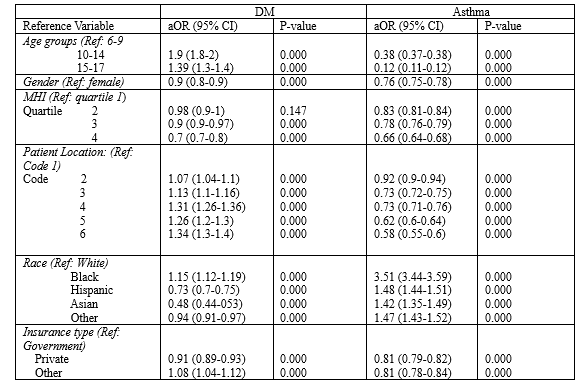 OR= Odds Ratio; Patient location:: 1- Central counties of metro areas of >=1 M population; 2- Fringe counties of metro areas of >=1 million population; 3- Counties in metro areas of 250,000-999,999 population; 4- Counties in metro areas of 50,000-249,999 population; 5- Micropolitan counties; 6- Not metropolitan or micropolitan counties
OR= Odds Ratio; Patient location:: 1- Central counties of metro areas of >=1 M population; 2- Fringe counties of metro areas of >=1 million population; 3- Counties in metro areas of 250,000-999,999 population; 4- Counties in metro areas of 50,000-249,999 population; 5- Micropolitan counties; 6- Not metropolitan or micropolitan counties