
Emergency Medicine 13
Session: Emergency Medicine 13
 Credit")

Alexandria Wiersma, MD
Assistant Professor, Pediatric Emergency Medicine
University of Colorado School of Medicine
Denver, Colorado, United States
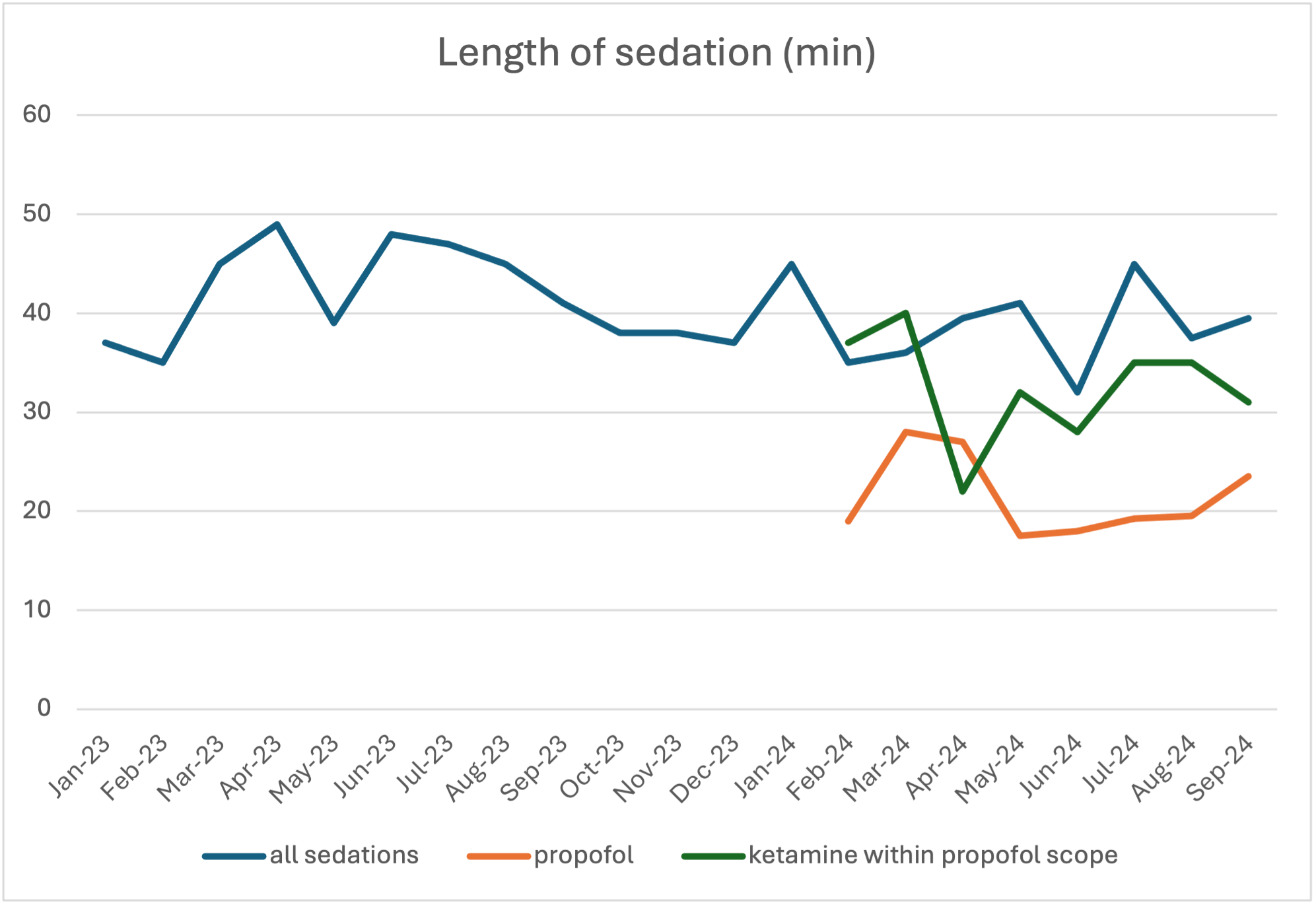 Comparing length of sedation (min) for all sedations, propofol sedations alone, and ketamine sedations within propofol scope
Comparing length of sedation (min) for all sedations, propofol sedations alone, and ketamine sedations within propofol scope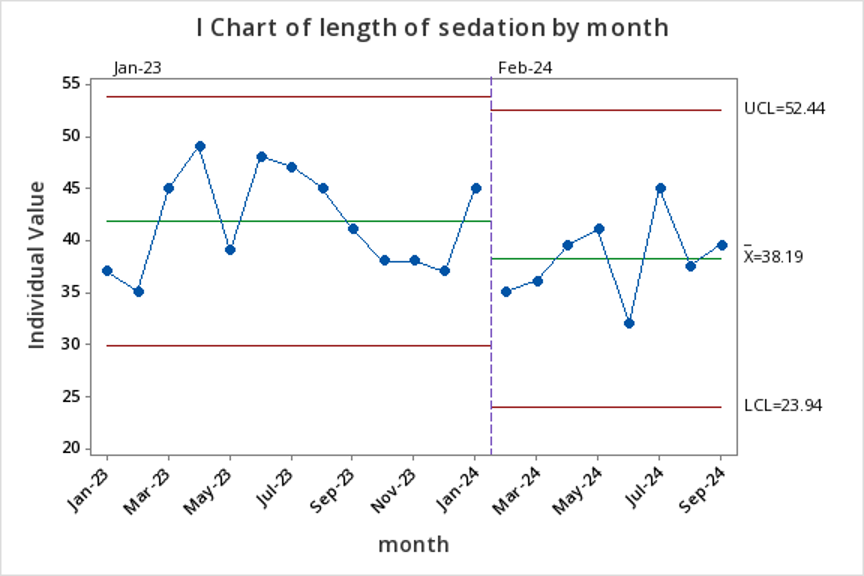 Pre and post intervention total length of sedation (all sedations)
Pre and post intervention total length of sedation (all sedations) Comparing length of sedation (min) for all sedations, propofol sedations alone, and ketamine sedations within propofol scopePre and post intervention total length of sedation (all sedations)
Comparing length of sedation (min) for all sedations, propofol sedations alone, and ketamine sedations within propofol scopePre and post intervention total length of sedation (all sedations)