
Neonatal Neurology 7: Pre-Clinical 1
Session: Neonatal Neurology 7: Pre-Clinical 1
 photo")
Joanne Davidson, PhD (she/her/hers)
Associate Professor
The University of Auckland
Auckland, Auckland, New Zealand
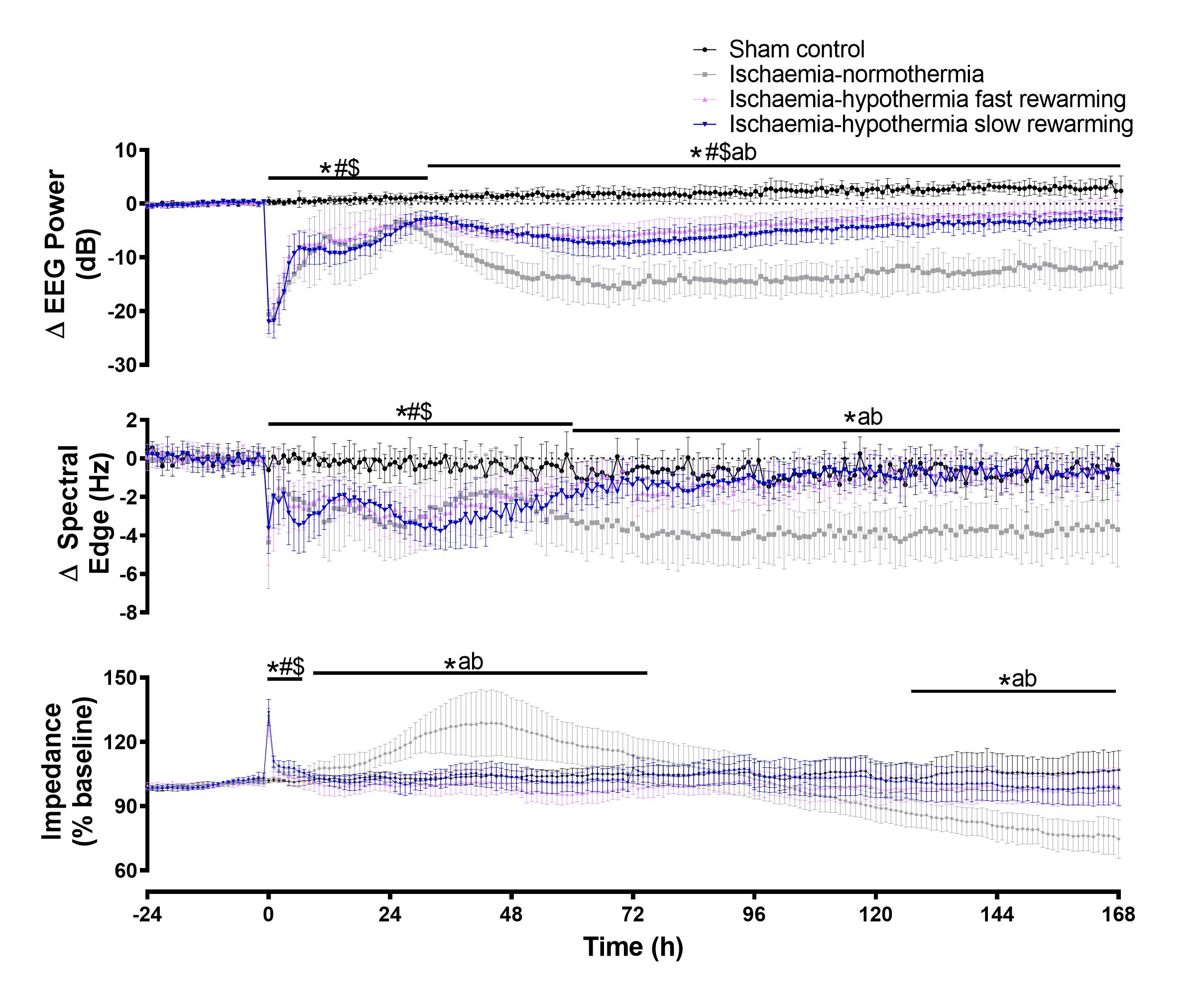 The rate of rewarming was not associated with any difference in recovery of EEG power, spectral edge frequency or cell swelling (impedance). * P<0.05 sham control vs. ischemia-normothermia, # P<0.05 sham control vs. ischemia-hypothermia fast rewarming, $ P<0.05 sham-control vs. ischemia-hypothermia slow rewarming, a P <0.05 ischemia-normothermia vs. ischemia-hypothermia fast rewarming, b P<0.05 ischemia-normothermia vs. ischemia-hypothermia slow rewarming.
The rate of rewarming was not associated with any difference in recovery of EEG power, spectral edge frequency or cell swelling (impedance). * P<0.05 sham control vs. ischemia-normothermia, # P<0.05 sham control vs. ischemia-hypothermia fast rewarming, $ P<0.05 sham-control vs. ischemia-hypothermia slow rewarming, a P <0.05 ischemia-normothermia vs. ischemia-hypothermia fast rewarming, b P<0.05 ischemia-normothermia vs. ischemia-hypothermia slow rewarming.