Neonatal General 11
Session: Neonatal General 11
 photo")
Elva Horath, MD (she/her/hers)
Pediatric Telehealth Project Policy Analyst
University of California Davis Children's Hospital
Citrus Heights, California, United States
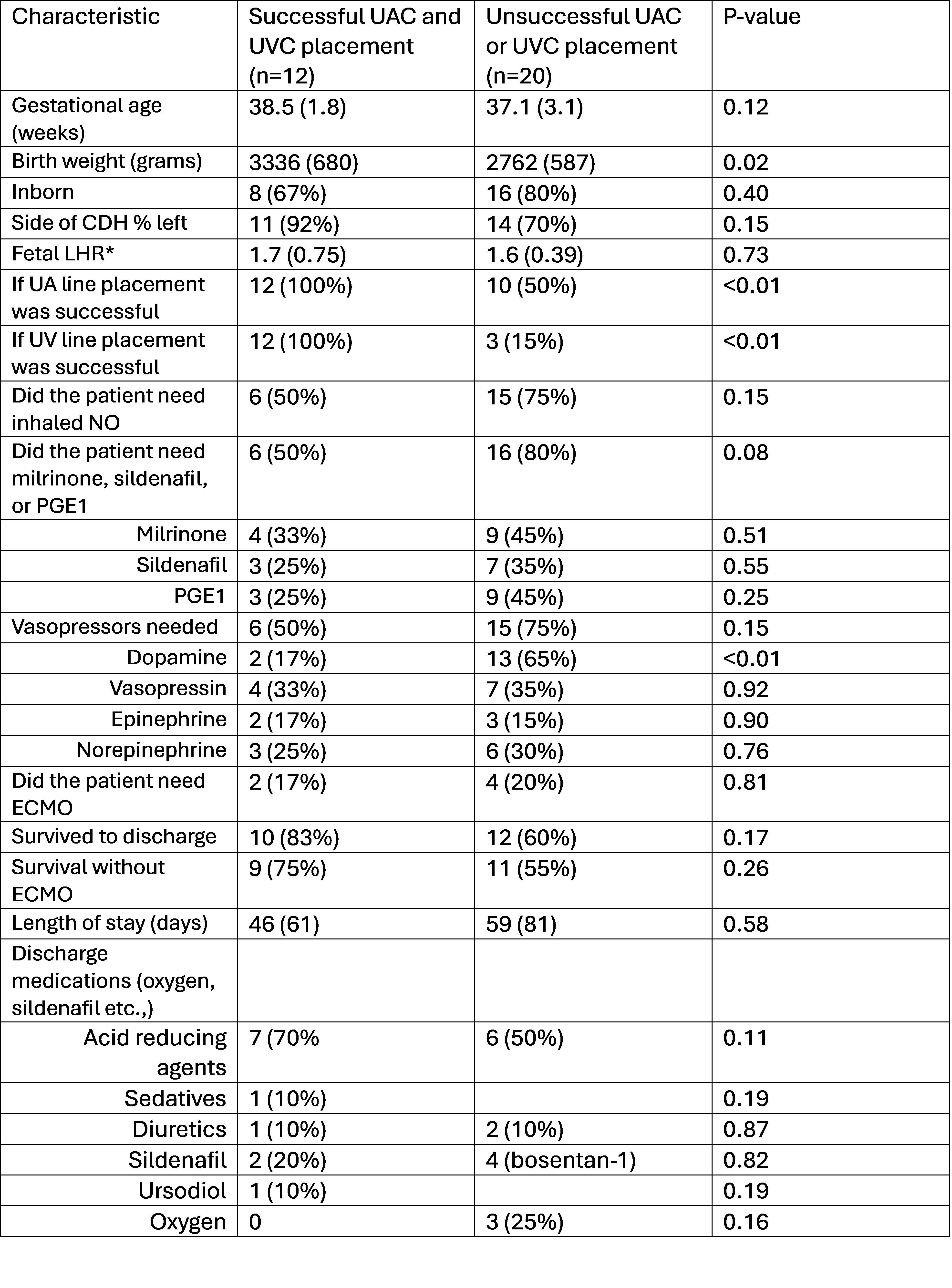 *Fetal LHR data only available 12 patients (6 in each group)
*Fetal LHR data only available 12 patients (6 in each group) *Fetal LHR data only available 12 patients (6 in each group)
*Fetal LHR data only available 12 patients (6 in each group)