
Neonatal Fetal Nutrition & Metabolism 4
Session: Neonatal Fetal Nutrition & Metabolism 4
Fumie Hojo
fellow
Japanese Red Cross Aichi Medical Center Nagoya Daini Hospital
Nagoya, Aichi, Japan
.jpg) Values are shown as median (range).
Values are shown as median (range).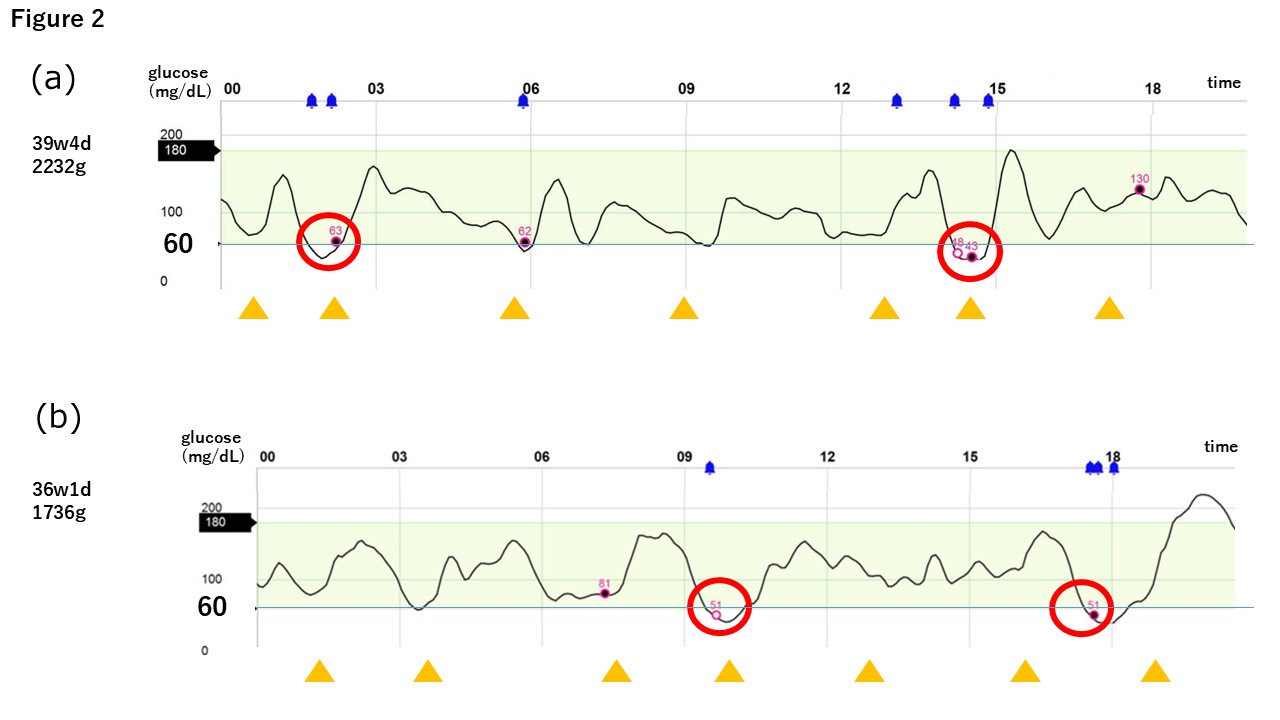 Yellow triangle: feeding; blue bell: low glucose level alert during CGM; pink point: low glucose level during self-monitoring of blood glucose; red circle: low-glucose event.
Yellow triangle: feeding; blue bell: low glucose level alert during CGM; pink point: low glucose level during self-monitoring of blood glucose; red circle: low-glucose event.