Neonatal/Infant Resuscitation 3
Session: Neonatal/Infant Resuscitation 3
Siyuan Jiang, jiangsiyuan@fudan.edu.cn (she/her/hers)
Children's Hospital of Fudan University
shanghai, Shanghai, China (People's Republic)
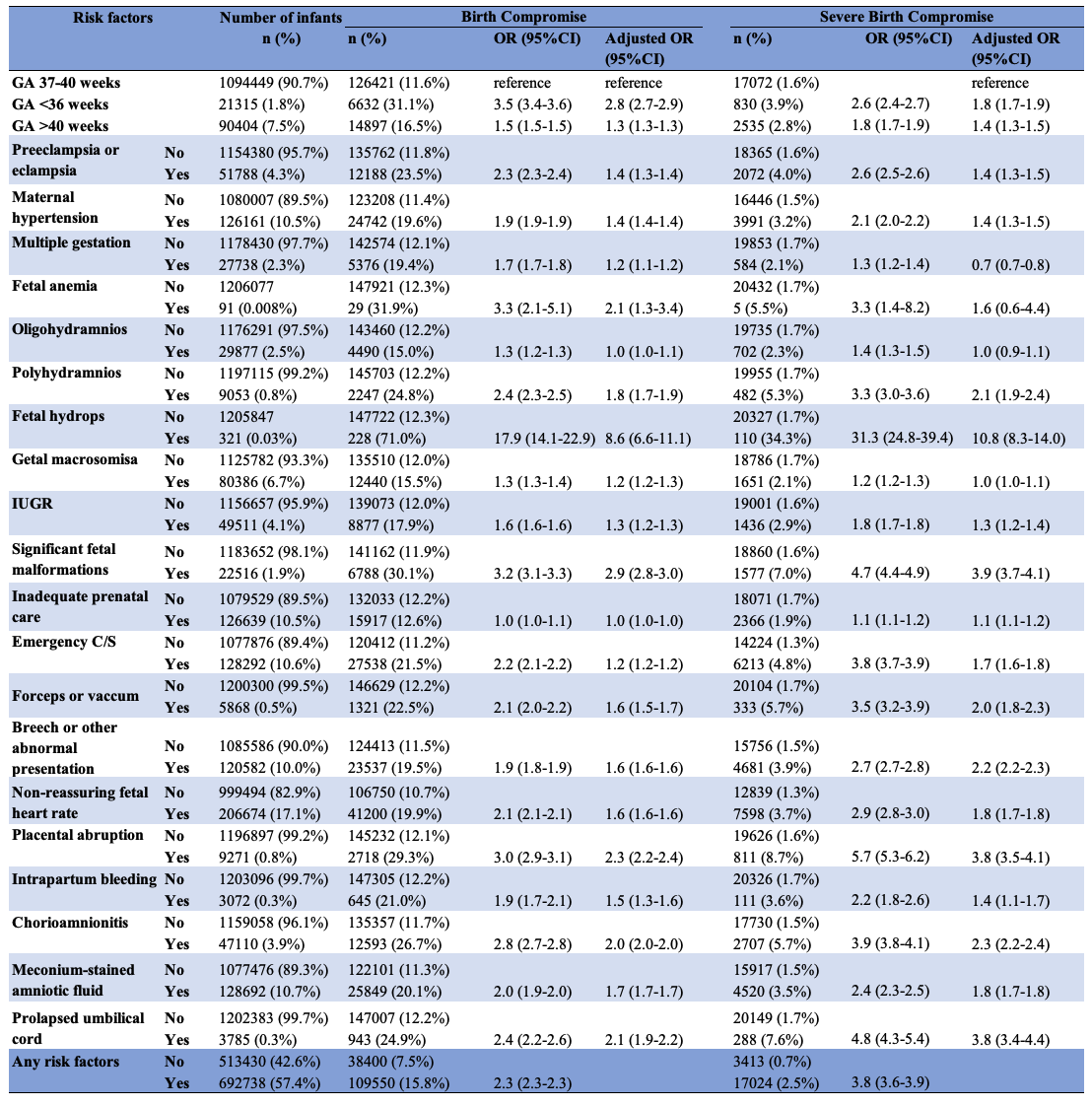
.png) Birth compromise was defined as any of the following: 1- or 5-minute Apgar score ≤7, death within 7 days, hypoxic-ischemic encephalopathy, acute respiratory disorders or respiratory support on day 1, and acute cardiovascular disorders or cardiovascular support on day 1.
Birth compromise was defined as any of the following: 1- or 5-minute Apgar score ≤7, death within 7 days, hypoxic-ischemic encephalopathy, acute respiratory disorders or respiratory support on day 1, and acute cardiovascular disorders or cardiovascular support on day 1.