706 - Optimal Timing of Ostomy Reversal in Preterm Neonates with Surgical Necrotizing Enterocolitis
Monday, April 28, 2025
7:00am - 9:15am HST
Publication Number: 706.6027
Dwayne Mascarenhas, The Hospital for Sick Children, Toronto, ON, Canada; Shravan Kanaparthi, The Hospital for Sick Children, Toronto, ON, Canada; Jordan Mann, The Hospital for Sick Children, Toronto, ON, Canada; Telford Yeung, University of Calgary, Calgary, AB, Canada; Mary A. Woodward, The Hospital for Sick Children, Toronto, ON, Canada; Bonny Jasani, The Hospital for Sick Children, Toronto, ON, Canada
Clinical Fellow The Hospital for Sick Children Toronto, Ontario, Canada
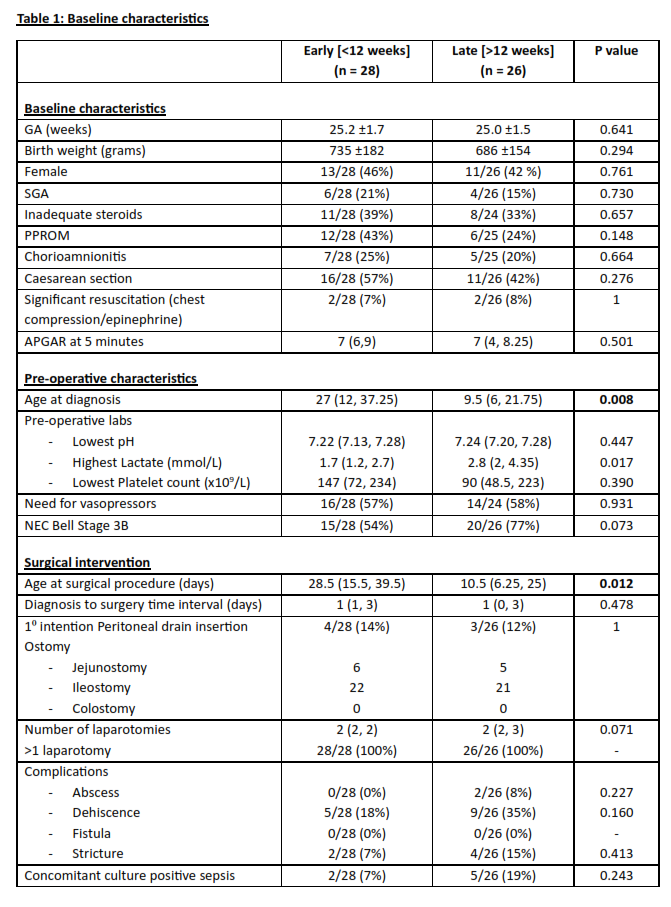
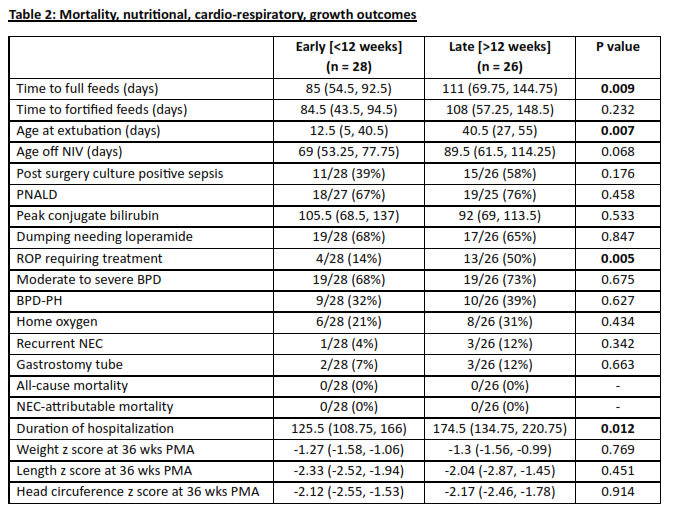
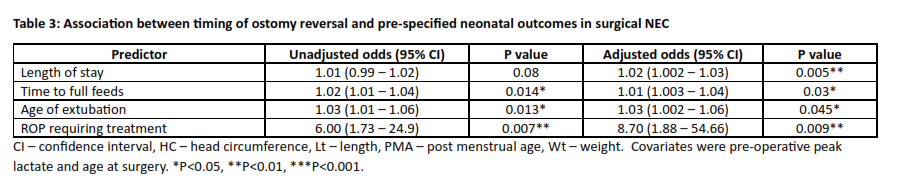
Background: Ostomy with or without mucous fistula is the standard of care in the management of surgical necrotizing enterocolitis (sNEC) in preterm infants. There is significant variability and lack of consensus on the optimal timing of ostomy reversal post-sNEC in preterm neonates. Objective: To evaluate the short-term outcomes in preterm infants whose ostomy was reversed early ( < 12 weeks) versus late (>12 weeks). Design/Methods: We conducted a retrospective cohort study of preterm infants ≤30 weeks with sNEC at a single quaternary neonatal intensive care unit between January 1, 2016 and June 30, 2024 who underwent ostomy reversal. The pre-specified outcomes included mortality (NEC-attributable and all-cause), need for >1 laparotomy, post-procedural complications, nutritional outcomes, neonatal morbidities, anthropometric indices (weight, length, head circumference z-scores) at 36 weeks postmenstrual age. Mann-Whitney U test and Fisher’s exact test were used for comparing continuous and categorical data respectively between the two groups. Multi-logistic regression analysis was conducted to compare the outcomes between the two groups, adjusted for confounders. Results: Of the 139 preterm infants with sNEC, 79 (57%) infants underwent ostomy. Of these, 54/79 (68%) neonates underwent reversal either early (n=28) or late (n=26). The baseline characteristics, details of surgical intervention, neonatal morbidities, and nutritional and anthropometric outcomes are outlined in Table 1. Compared to the early ostomy reversal group, the infants in the late ostomy reversal group had higher time to reach full feeds (111 vs 85 days; p=0.009), later age at extubation (40.5 vs 12.5 days; p=0.007), higher need for treatment of ROP (50 vs 14%; p= 0.005), and longer duration of hospitalization (174.4 vs 125.5 days; p=0.012) (Table 2). Post-adjusted analysis, the odds of duration of hospitalization, time to full feeds, age at extubation, ROP requiring treatment were significantly lower in early ostomy reversal group compared to late ostomy reversal group (Table 3).
Conclusion(s): Our study showed that early ostomy reversal may have numerous advantages compared to late ostomy reversal in preterm sNEC without an increase in complications. Standardization of timing of ostomy reversal should be the focus of quality improvement initiatives to reduce the burden of morbidities and hospitalization in preterm neonates with sNEC.

.jpg "Dwayne Mascarenhas, MBBS, MD (Paeds), DM (Neonatology) (he/him/his) photo")