
Neonatal General 11
Session: Neonatal General 11
Spencer Millen, MD (he/him/his)
Neonatology Fellow
Ann & Robert H. Lurie Children's Hospital of Chicago
469 W Huron St, Illinois, United States
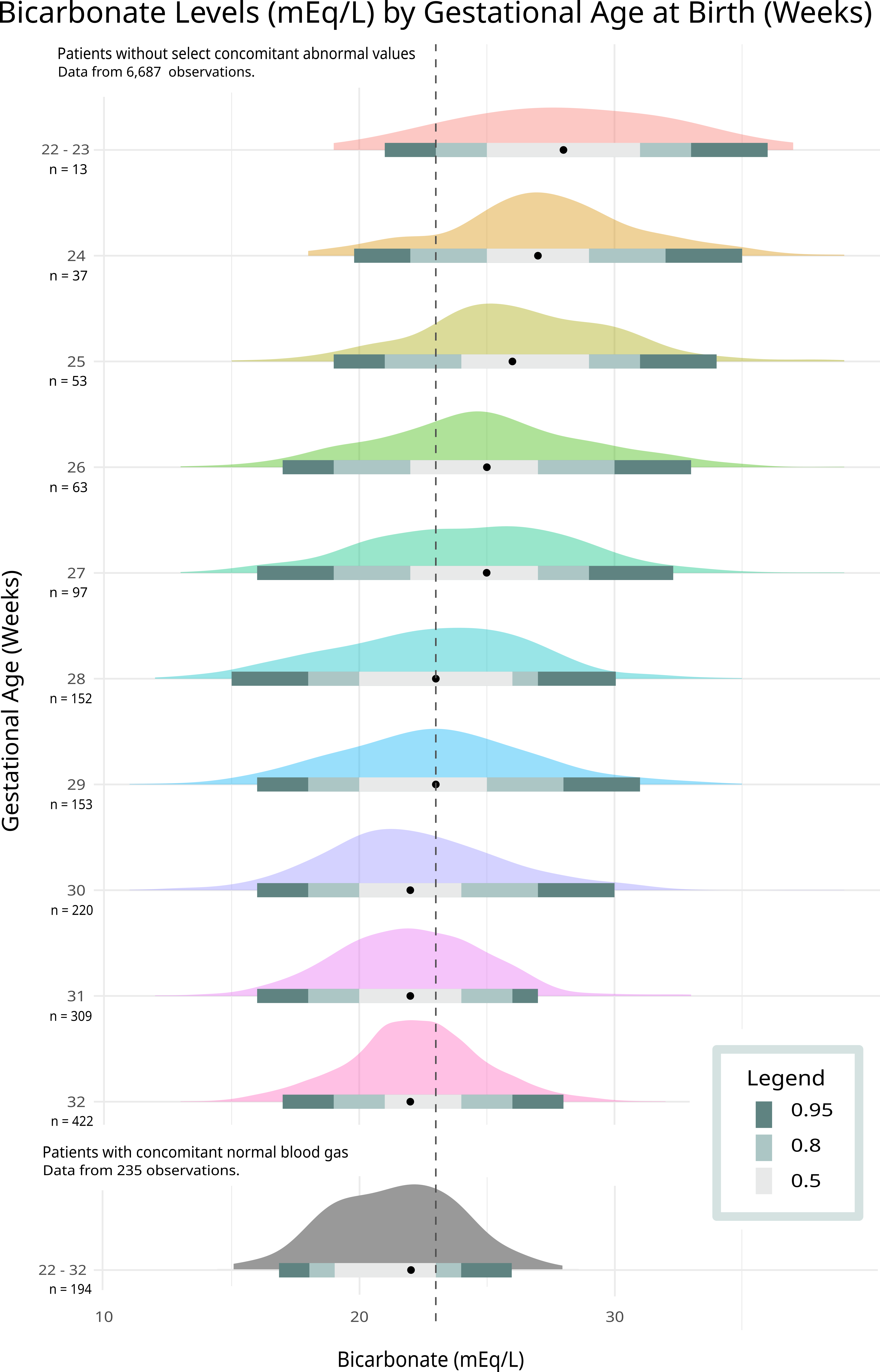 Measurements of bicarbonate were recorded throughout a patient’s NICU admission. Each included measurement occurred without a recorded abnormal Na+, K+, pCO2, pH, creatinine, or elevated Lactate within 12 hours before or after. The legend denotes 50th, 80th, and 95th percentile distribution of lab values. 235 measurements from 194 patients had a bicarbonate measurement within 1 hour of a normal blood gas. The distribution of this restrictive inclusion criteria is displayed in grey.
Measurements of bicarbonate were recorded throughout a patient’s NICU admission. Each included measurement occurred without a recorded abnormal Na+, K+, pCO2, pH, creatinine, or elevated Lactate within 12 hours before or after. The legend denotes 50th, 80th, and 95th percentile distribution of lab values. 235 measurements from 194 patients had a bicarbonate measurement within 1 hour of a normal blood gas. The distribution of this restrictive inclusion criteria is displayed in grey.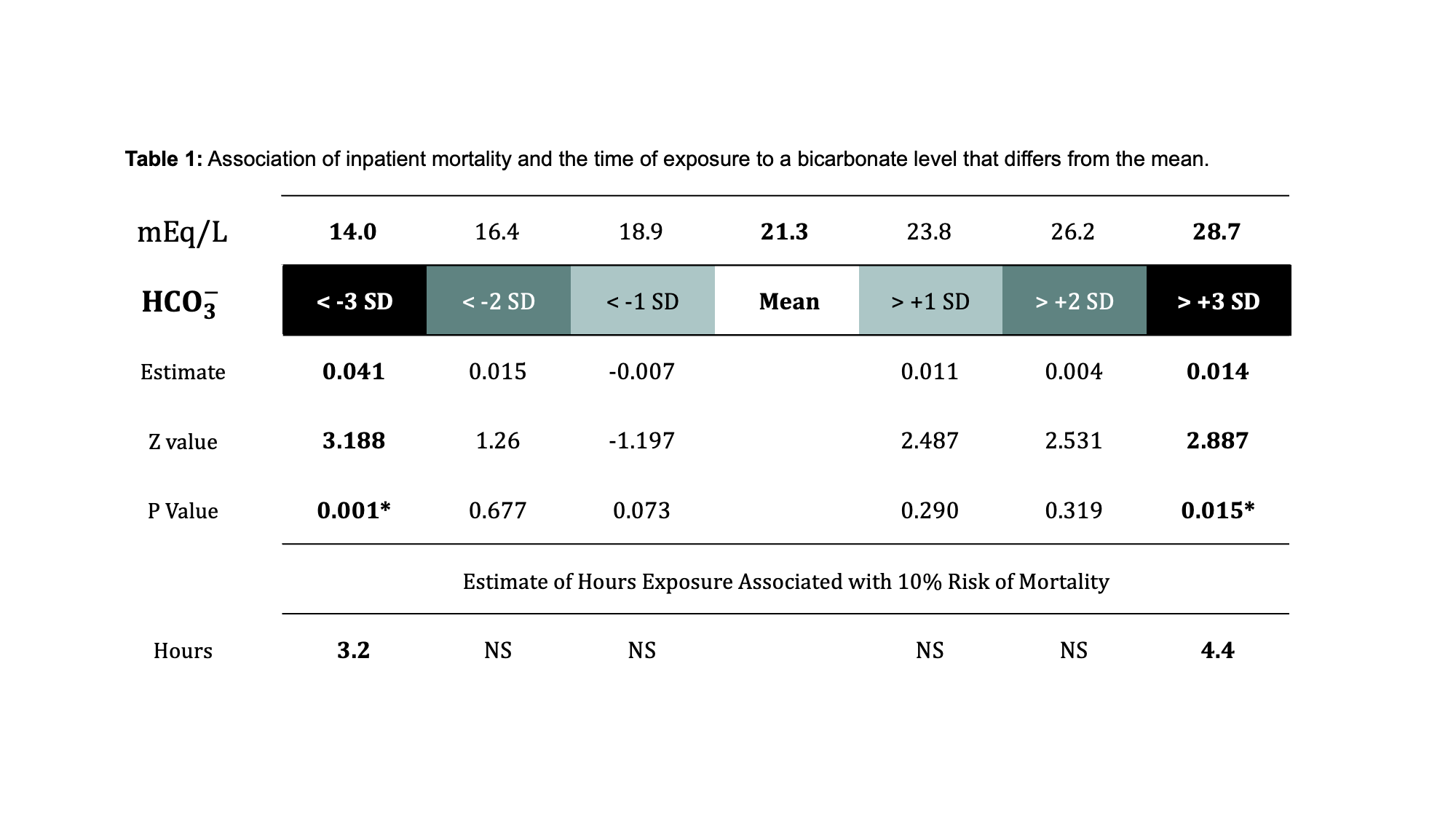 Each hour of life above or below the designated threshold was tallied representing the estimated time of exposure. The univariate logistic regression compared hours of exposure to inpatient mortality. (NS, Non-significant)
Each hour of life above or below the designated threshold was tallied representing the estimated time of exposure. The univariate logistic regression compared hours of exposure to inpatient mortality. (NS, Non-significant)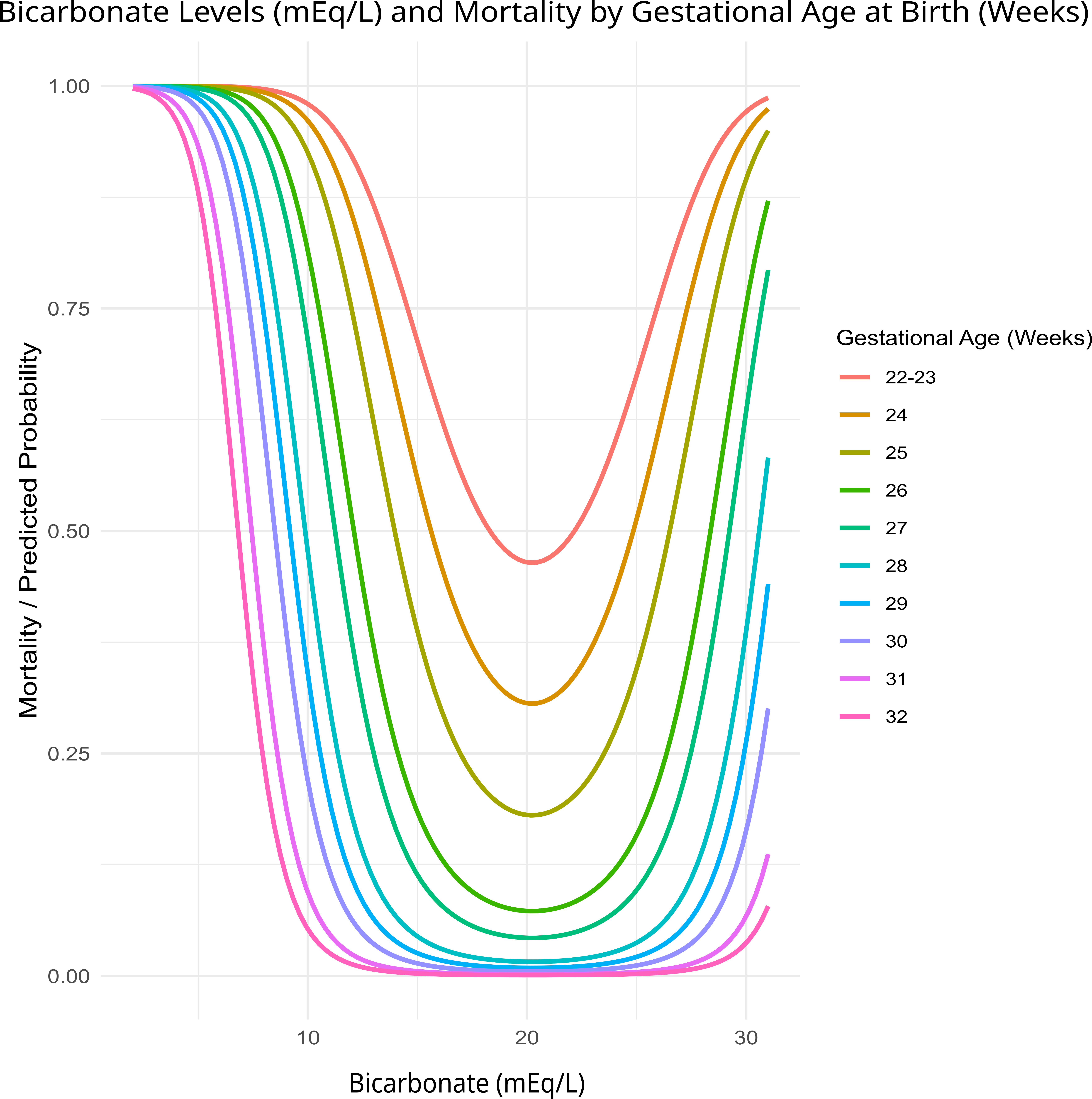 A quadratic transformation was applied to allow appropriate fit. Principal component analysis consisted of gestational age, sex, birthweight, and Apgar score. Using this multivariable, generalized quadratic model, the associated mortality was estimated with simulated bicarbonate values and gestational age. The HCO₃⁻ value associated with the minimum inpatient mortality risk is 21.2 mEq/L.
A quadratic transformation was applied to allow appropriate fit. Principal component analysis consisted of gestational age, sex, birthweight, and Apgar score. Using this multivariable, generalized quadratic model, the associated mortality was estimated with simulated bicarbonate values and gestational age. The HCO₃⁻ value associated with the minimum inpatient mortality risk is 21.2 mEq/L. 