
Neonatal Fetal Nutrition & Metabolism 4
Session: Neonatal Fetal Nutrition & Metabolism 4
William King, MSEE (he/him/his)
CEO
Medical Predictive Science Corporation
Charlottesville, Virginia, United States
 Patient demographics. Data are expressed as Median [IQR] or Count (Percent).
Patient demographics. Data are expressed as Median [IQR] or Count (Percent).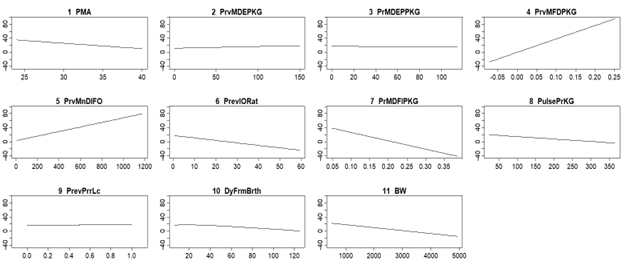 Model response to predictor variables. Y-axis is modeled weight gain per KG per day over the previous seven days. 1 PMA: Postmenstrual Age. 2 PrvMDEPKG: Previous Mean Daily Energy per KG. 3 PrMDEPPKG: Previous Mean Daily Parenteral Energy per KG. 4 PrvMFDPKG: Previous Mean Fluid I/O Difference per KG. 5 PrvMnDlFO: Previous Mean Daily Fluid Output. 6 PrevIORat: Previous I/O Ratio. 7 PrMDFIPerKG: Previous Mean Daily Fluid Intake per KG. 8 PulsePrPG: Pulse per KG. 9 PrevPrrLc: Previous Prior Location (e.g. surgery). 10 DyFrmBrth: Day From Birth. 11 BW: Birth weight.
Model response to predictor variables. Y-axis is modeled weight gain per KG per day over the previous seven days. 1 PMA: Postmenstrual Age. 2 PrvMDEPKG: Previous Mean Daily Energy per KG. 3 PrMDEPPKG: Previous Mean Daily Parenteral Energy per KG. 4 PrvMFDPKG: Previous Mean Fluid I/O Difference per KG. 5 PrvMnDlFO: Previous Mean Daily Fluid Output. 6 PrevIORat: Previous I/O Ratio. 7 PrMDFIPerKG: Previous Mean Daily Fluid Intake per KG. 8 PulsePrPG: Pulse per KG. 9 PrevPrrLc: Previous Prior Location (e.g. surgery). 10 DyFrmBrth: Day From Birth. 11 BW: Birth weight.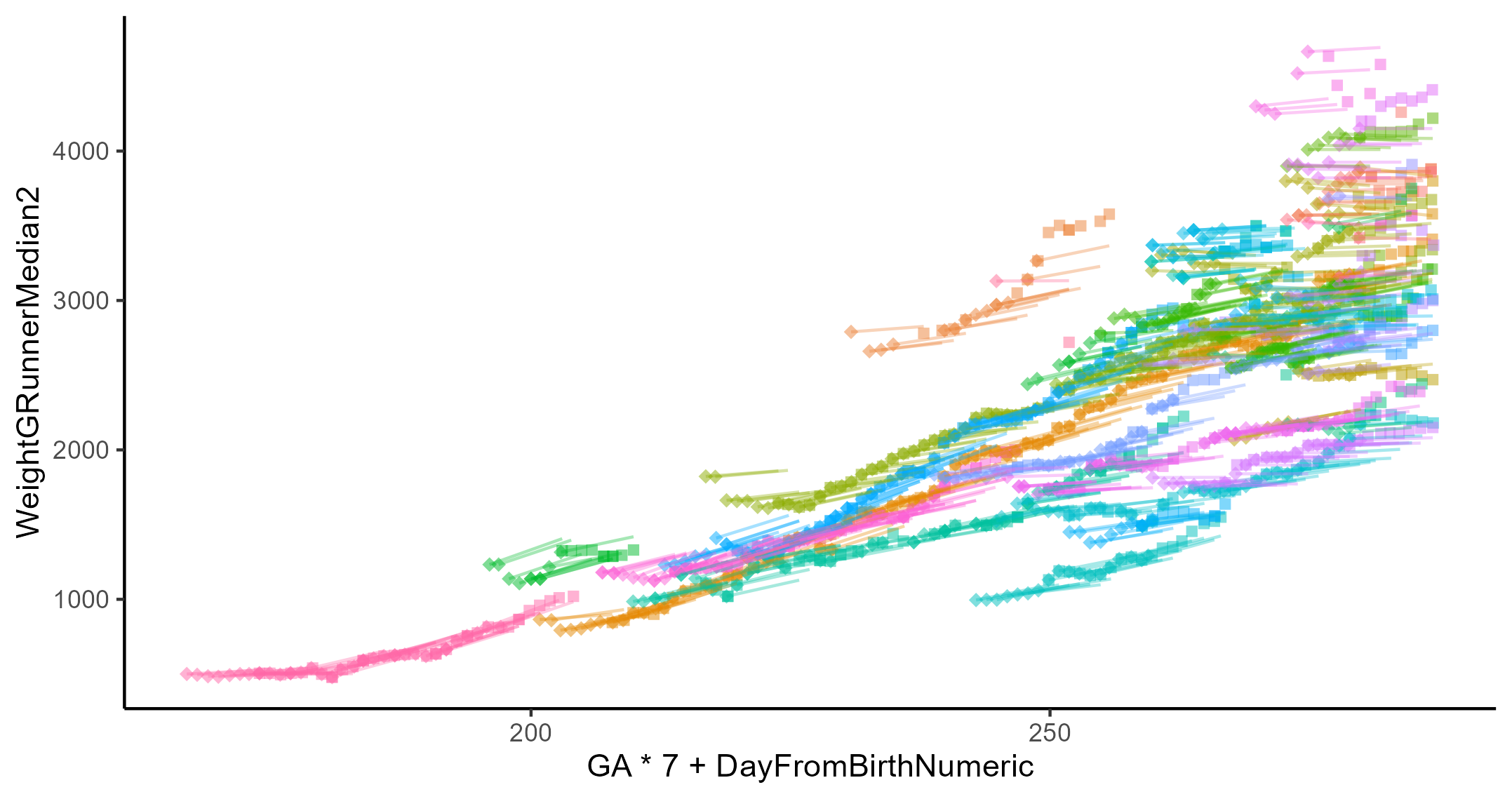 Growth plot of approximately sixty patients. The diamonds and squares represent the beginning and end, respectively, of a 7-day period with recorded weight on both ends. While the line represents modeled growth over the same 7-day span. The x-axis the post menstrual age.
Growth plot of approximately sixty patients. The diamonds and squares represent the beginning and end, respectively, of a 7-day period with recorded weight on both ends. While the line represents modeled growth over the same 7-day span. The x-axis the post menstrual age.