
Neonatal Neurology 7: Pre-Clinical 1
Session: Neonatal Neurology 7: Pre-Clinical 1
 photo")
Joanne Davidson, PhD (she/her/hers)
Associate Professor
The University of Auckland
Auckland, Auckland, New Zealand
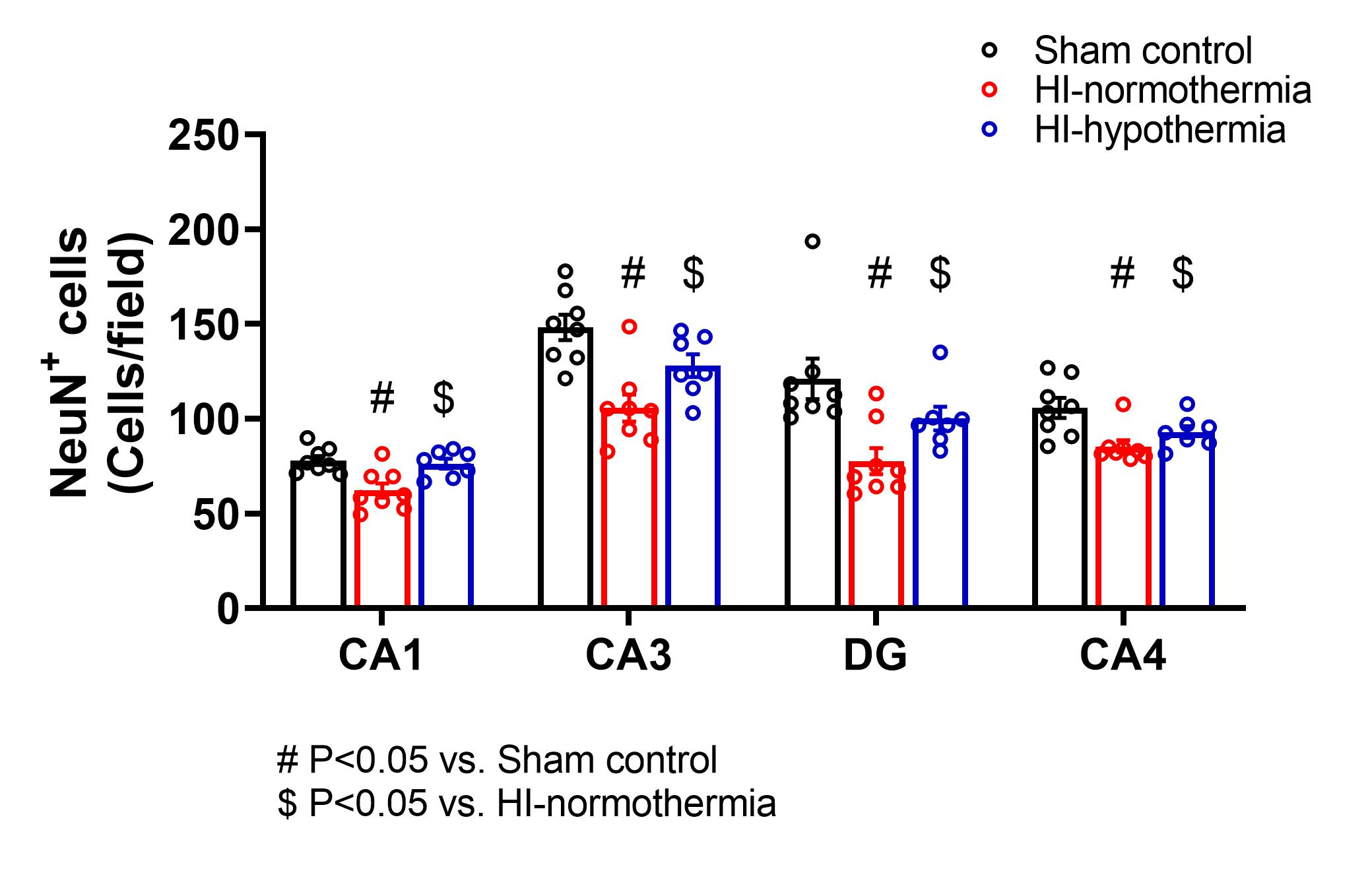 Ischemia was associated with a significant decrease in neuron numbers in all regions of the hippocampus, while therapeutic hypothermia significantly increased neuron number back to sham control level.
Ischemia was associated with a significant decrease in neuron numbers in all regions of the hippocampus, while therapeutic hypothermia significantly increased neuron number back to sham control level.