
Neonatal/Infant Resuscitation 4
Session: Neonatal/Infant Resuscitation 4
 photo")
Marcus J. Donnelly, MD Candidate (he/him/his)
Medical Student
University of North Carolina at Chapel Hill School of Medicine
Chapel Hill, North Carolina, United States
.png) A) Event registration screen of the Liveborn app: In real-time, an observer uses Liveborn to record the start and stop times of key resuscitation actions including stimulation, suction, and ventilation. B) Resuscitation station with AV recording: When a newborn is moved to the warmer for resuscitation, the observer initiates AV recording via a mounted tablet.
A) Event registration screen of the Liveborn app: In real-time, an observer uses Liveborn to record the start and stop times of key resuscitation actions including stimulation, suction, and ventilation. B) Resuscitation station with AV recording: When a newborn is moved to the warmer for resuscitation, the observer initiates AV recording via a mounted tablet. .png)
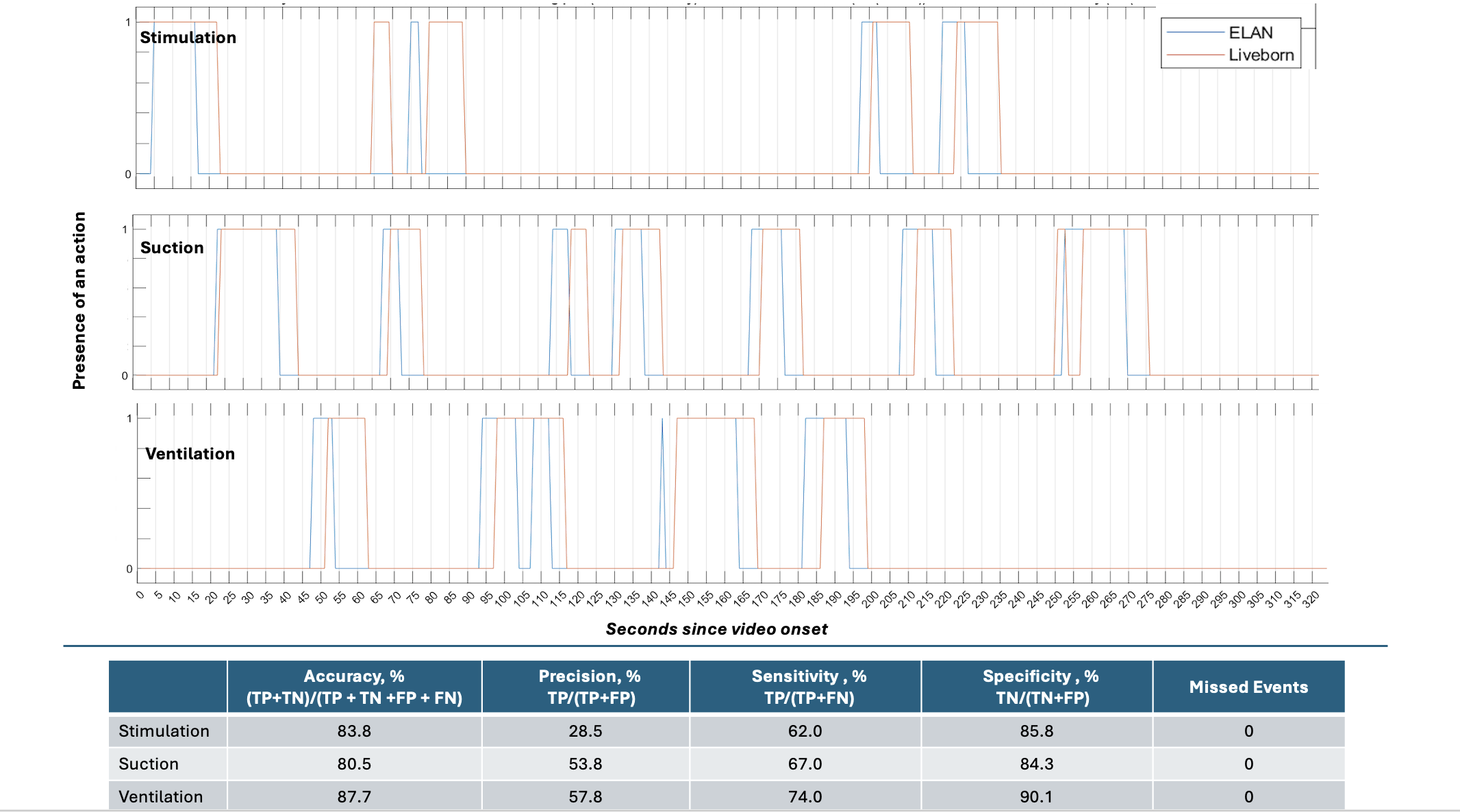 The plots depict the frequency of stimulation, suctioning and ventilation for one case of resuscitation with annotations of AV-recorded data depicted in blue and real-time observation with Liveborn depicted in orange. Accuracy represents the proportion of time the observer documented what was actually happening. Precision represents the proportion of time the observer’s documentation of suctioning was actually true, i.e., avoiding false detection of suctioning. Sensitivity represents the proportion of actual time spent suctioning that was documented by the observer, i.e., not missing suctioning. Specificity represents the proportion of actual time not suctioning that was documented by the observer, i.e., documenting the absence of suctioning. Abbreviations: AV=audio video; FN=false negative; FP=false positive; TN=true negative; TP=true positive. A) Event registration screen of the Liveborn app: In real-time, an observer uses Liveborn to record the start and stop times of key resuscitation actions including stimulation, suction, and ventilation. B) Resuscitation station with AV recording: When a newborn is moved to the warmer for resuscitation, the observer initiates AV recording via a mounted tablet. The plots depict the frequency of stimulation, suctioning and ventilation for one case of resuscitation with annotations of AV-recorded data depicted in blue and real-time observation with Liveborn depicted in orange. Accuracy represents the proportion of time the observer documented what was actually happening. Precision represents the proportion of time the observer’s documentation of suctioning was actually true, i.e., avoiding false detection of suctioning. Sensitivity represents the proportion of actual time spent suctioning that was documented by the observer, i.e., not missing suctioning. Specificity represents the proportion of actual time not suctioning that was documented by the observer, i.e., documenting the absence of suctioning. Abbreviations: AV=audio video; FN=false negative; FP=false positive; TN=true negative; TP=true positive.
The plots depict the frequency of stimulation, suctioning and ventilation for one case of resuscitation with annotations of AV-recorded data depicted in blue and real-time observation with Liveborn depicted in orange. Accuracy represents the proportion of time the observer documented what was actually happening. Precision represents the proportion of time the observer’s documentation of suctioning was actually true, i.e., avoiding false detection of suctioning. Sensitivity represents the proportion of actual time spent suctioning that was documented by the observer, i.e., not missing suctioning. Specificity represents the proportion of actual time not suctioning that was documented by the observer, i.e., documenting the absence of suctioning. Abbreviations: AV=audio video; FN=false negative; FP=false positive; TN=true negative; TP=true positive. A) Event registration screen of the Liveborn app: In real-time, an observer uses Liveborn to record the start and stop times of key resuscitation actions including stimulation, suction, and ventilation. B) Resuscitation station with AV recording: When a newborn is moved to the warmer for resuscitation, the observer initiates AV recording via a mounted tablet. The plots depict the frequency of stimulation, suctioning and ventilation for one case of resuscitation with annotations of AV-recorded data depicted in blue and real-time observation with Liveborn depicted in orange. Accuracy represents the proportion of time the observer documented what was actually happening. Precision represents the proportion of time the observer’s documentation of suctioning was actually true, i.e., avoiding false detection of suctioning. Sensitivity represents the proportion of actual time spent suctioning that was documented by the observer, i.e., not missing suctioning. Specificity represents the proportion of actual time not suctioning that was documented by the observer, i.e., documenting the absence of suctioning. Abbreviations: AV=audio video; FN=false negative; FP=false positive; TN=true negative; TP=true positive. 