
Nephrology 5
Session: Nephrology 5
 Credit")

Daniel Rosenfeld, MD
Resident
K. Hovnanian Children’s Hospital at Jersey Shore University Medical Center
Asbury Park, New Jersey, United States
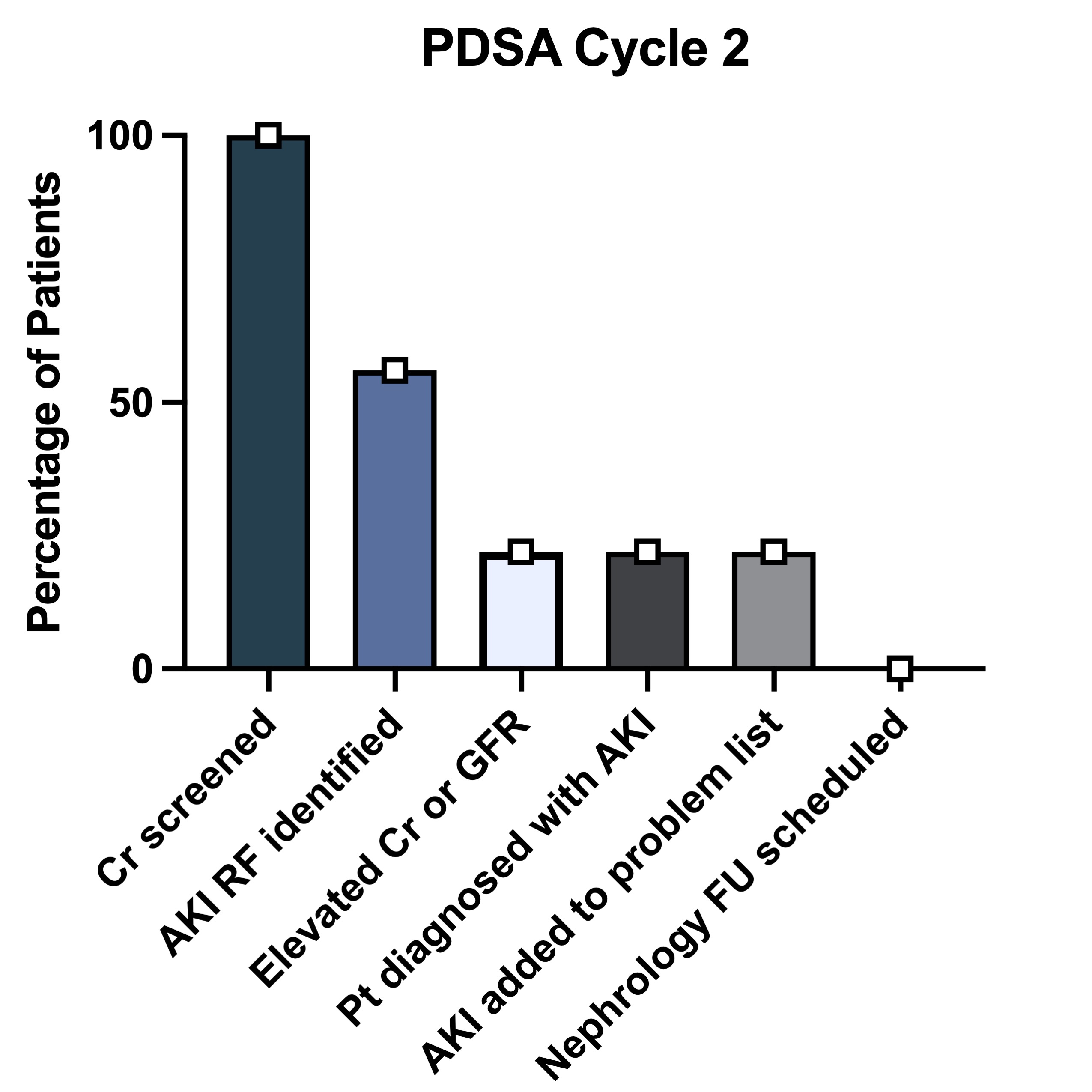 o AKI Screening Rate: Increased to 56%.
o AKI Screening Rate: Increased to 56%.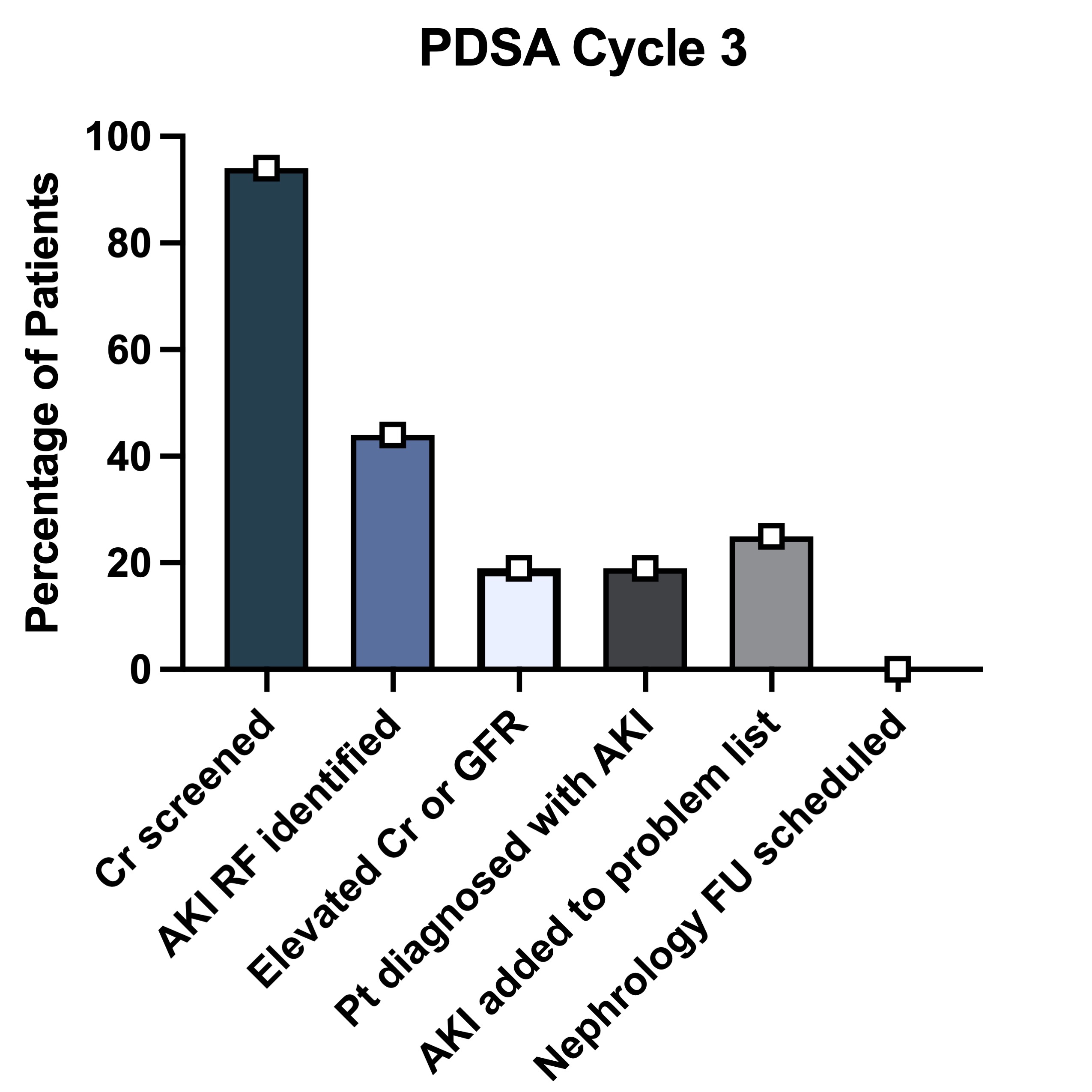 o AKI Screening Rate: Increased to 94%.
o AKI Screening Rate: Increased to 94%.