
Emergency Medicine 3
Session: Emergency Medicine 3
 photo")
Nathan M. Money, DO (he/him/his)
Assistant professor
University of Utah
Lehi, Utah, United States
.jpg) Inter-hospital variation among 16 hospitals in the care of hypothermic infants presenting to the emergency department. Median value is represented by the dark horizontal line, interquartile range by the shaded box area, and range by the vertical line.
Inter-hospital variation among 16 hospitals in the care of hypothermic infants presenting to the emergency department. Median value is represented by the dark horizontal line, interquartile range by the shaded box area, and range by the vertical line. 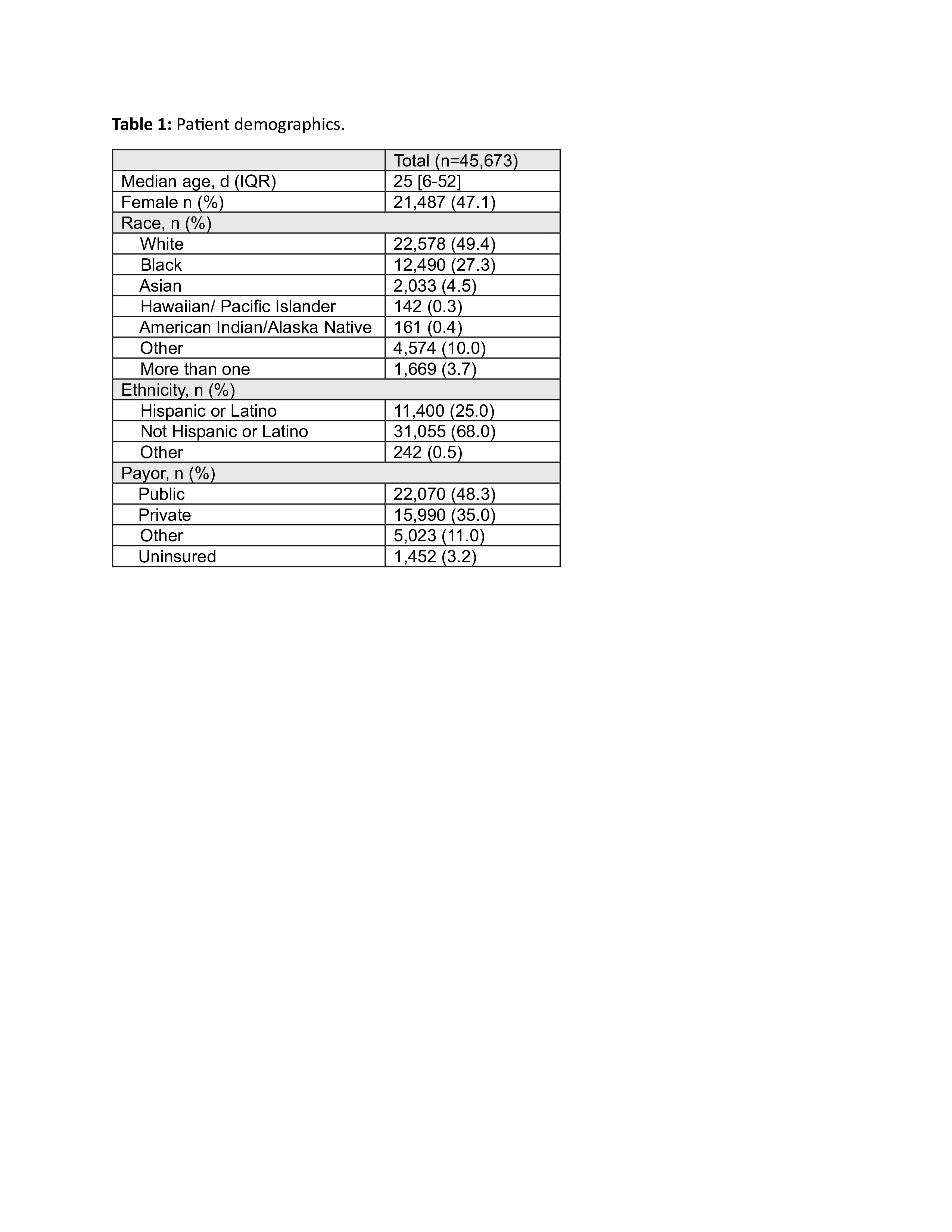 Patient demographics.
Patient demographics.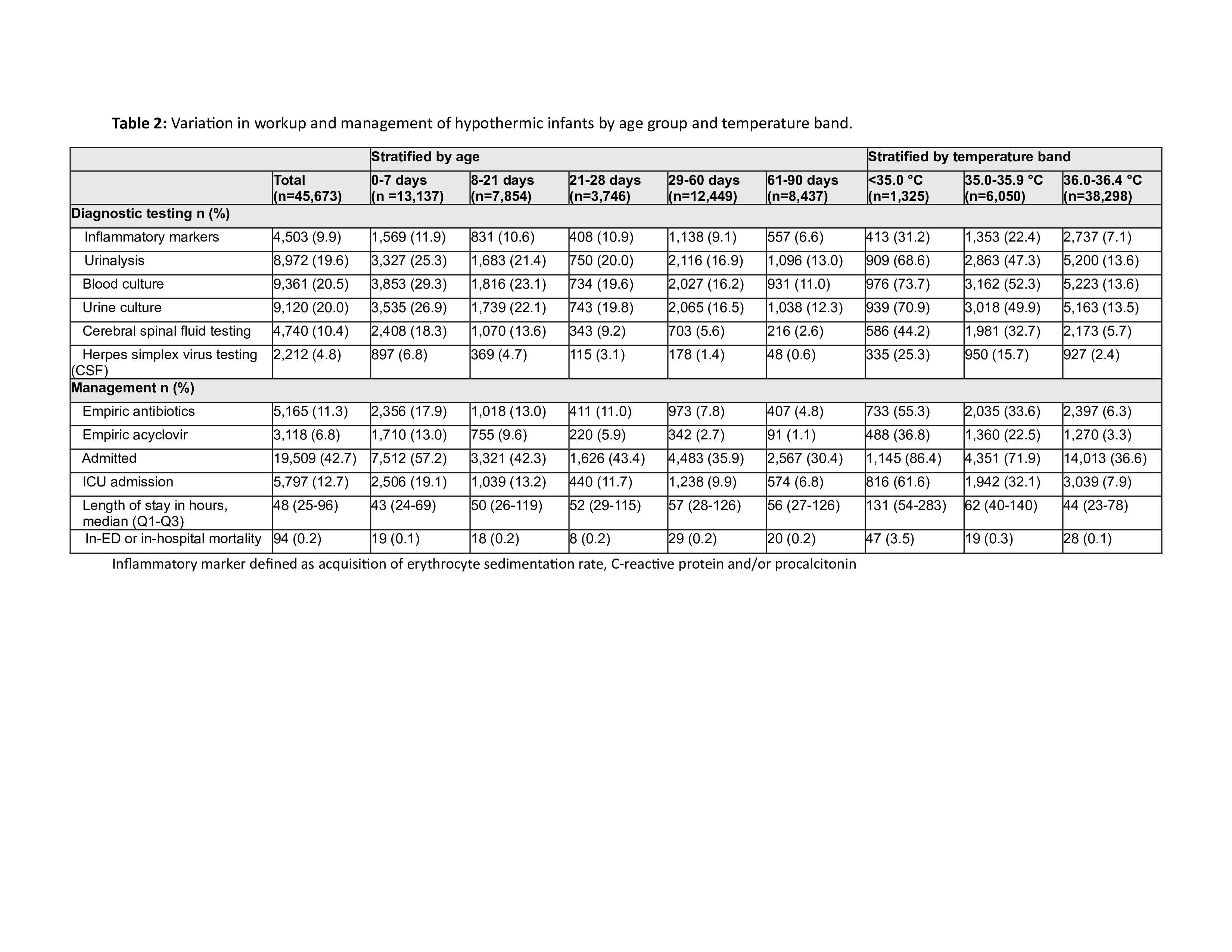 Variation in workup and management of hypothermic infants by age group and temperature band. Inter-hospital variation among 16 hospitals in the care of hypothermic infants presenting to the emergency department. Median value is represented by the dark horizontal line, interquartile range by the shaded box area, and range by the vertical line. Patient demographics.Variation in workup and management of hypothermic infants by age group and temperature band.
Variation in workup and management of hypothermic infants by age group and temperature band. Inter-hospital variation among 16 hospitals in the care of hypothermic infants presenting to the emergency department. Median value is represented by the dark horizontal line, interquartile range by the shaded box area, and range by the vertical line. Patient demographics.Variation in workup and management of hypothermic infants by age group and temperature band. 