
Critical Care 2
Session: Critical Care 2
 photo")
Sarah Jaffar, MD (she/her/hers)
Fellow Physician, Pediatric Critical Care
Children's National Health System
Washington, District of Columbia, United States
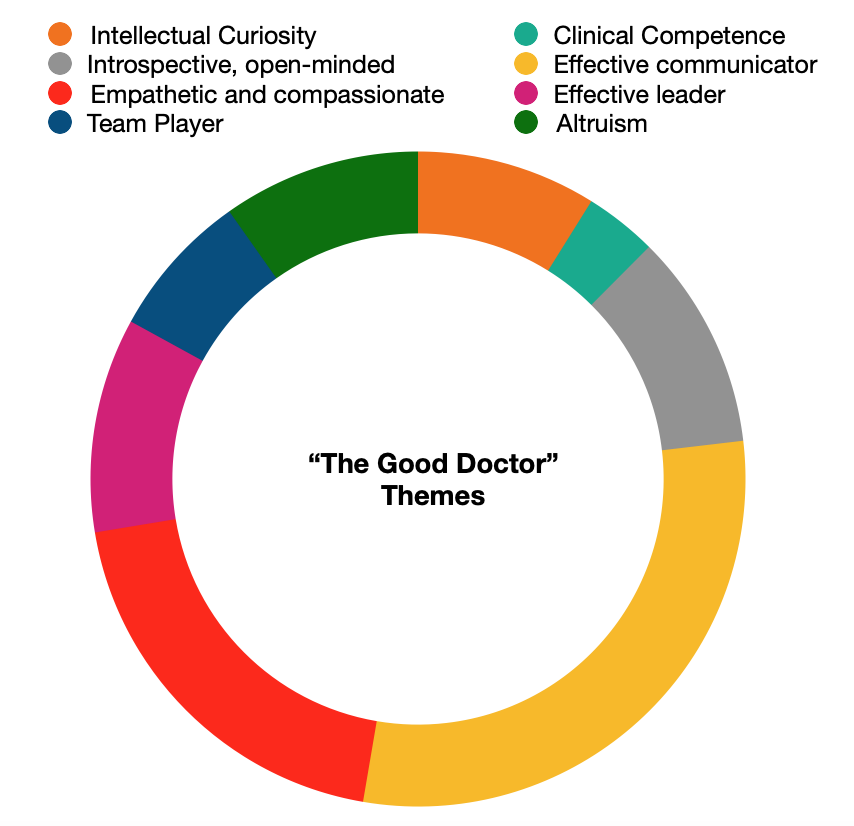 Clinician themes of "good doctor" characteristics qualitatively defined by ICU providers.
Clinician themes of "good doctor" characteristics qualitatively defined by ICU providers. 