
Critical Care 2
Session: Critical Care 2
 photo")
Sarah Kandil, MD (she/her/hers)
Associate Professor of Pediatrics
Yale University - Pediatrics
New Haven, Connecticut, United States
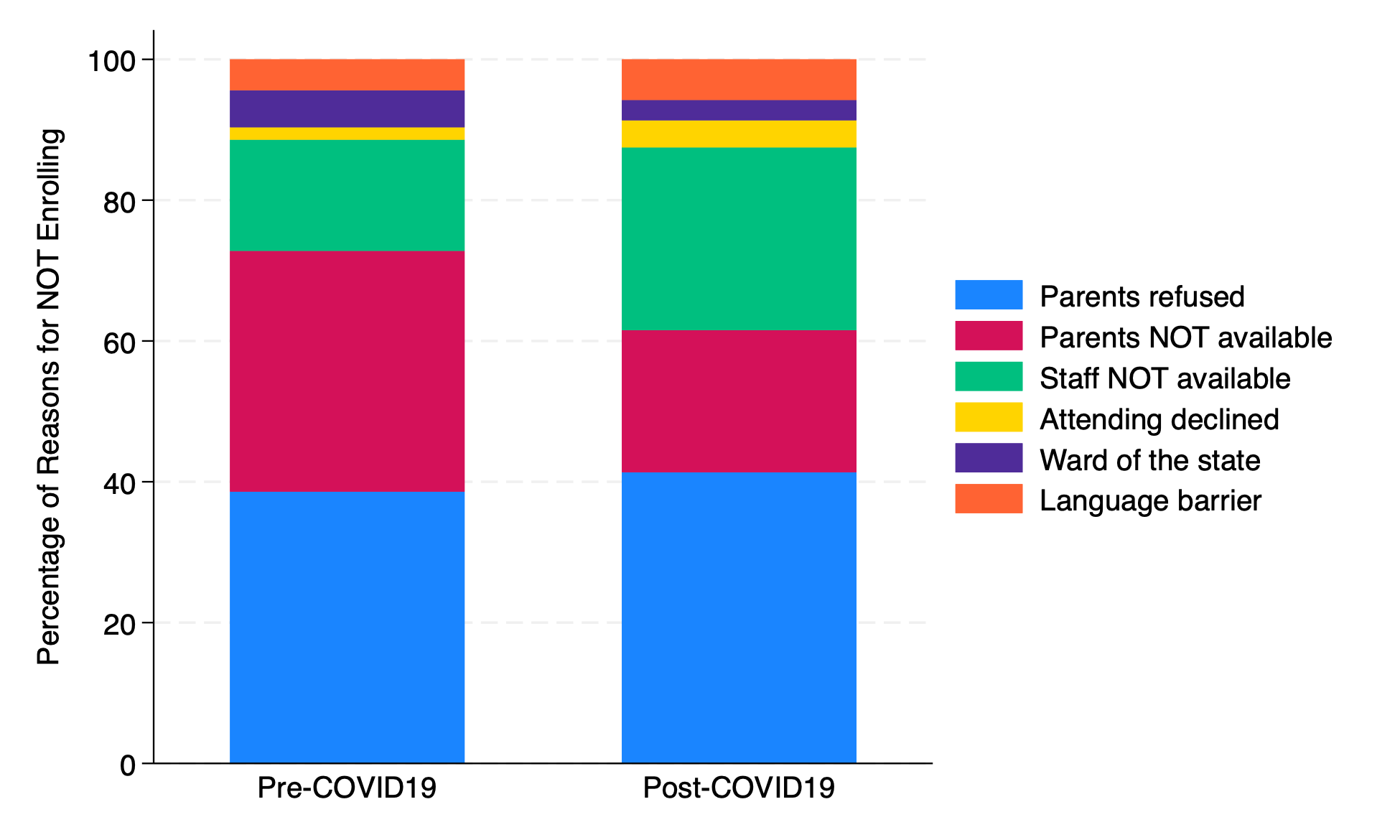 Stacked bar chart of reasons for not enrolling eligible children by enrollment period. The distribution of reasons for not enrolling these children was different pre- and post-COVID19.
Stacked bar chart of reasons for not enrolling eligible children by enrollment period. The distribution of reasons for not enrolling these children was different pre- and post-COVID19. 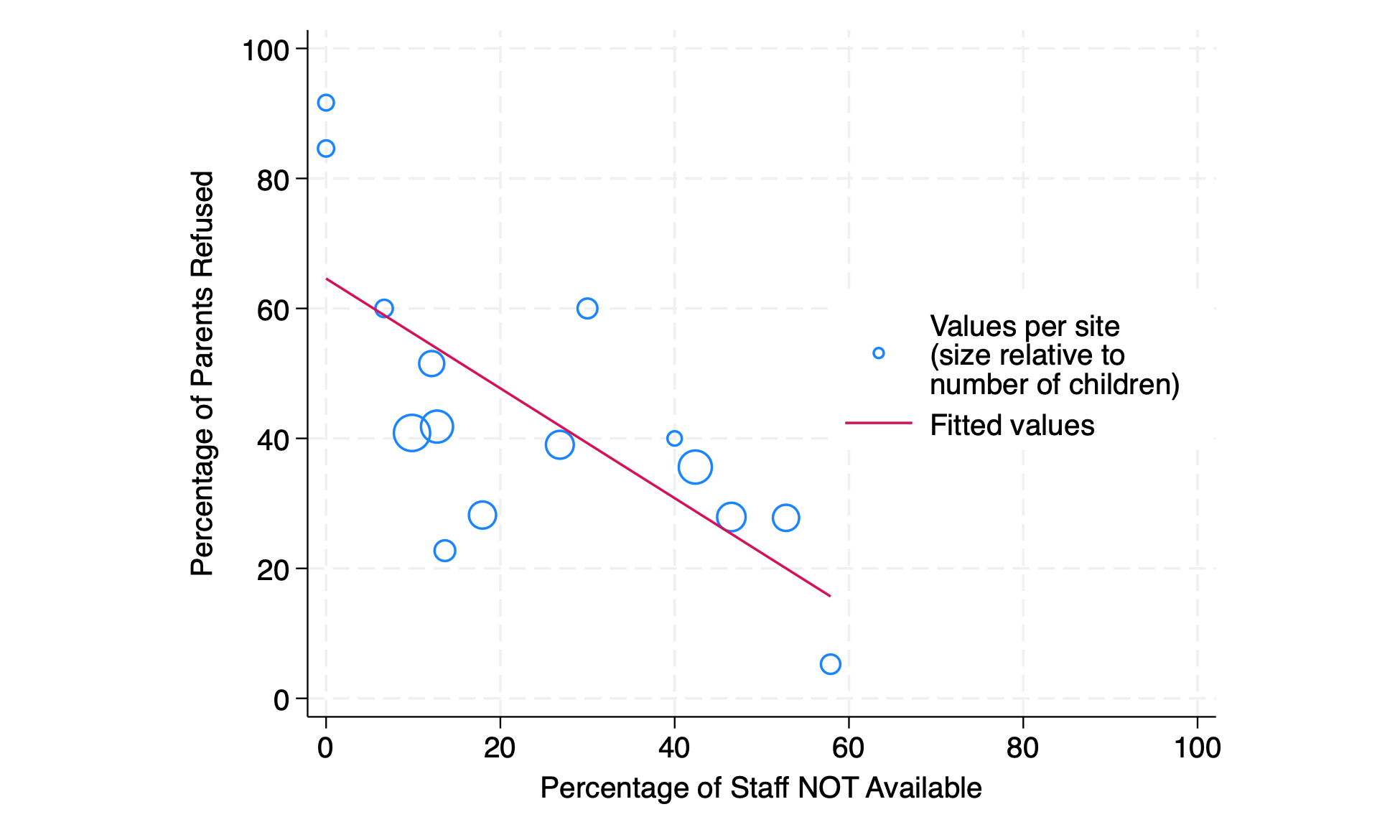 Scatterplot of parental refusal and research staff not available. The percentage of parental refusal per hospital was inversely correlated with the percentage of unavailability of research staff.
Scatterplot of parental refusal and research staff not available. The percentage of parental refusal per hospital was inversely correlated with the percentage of unavailability of research staff.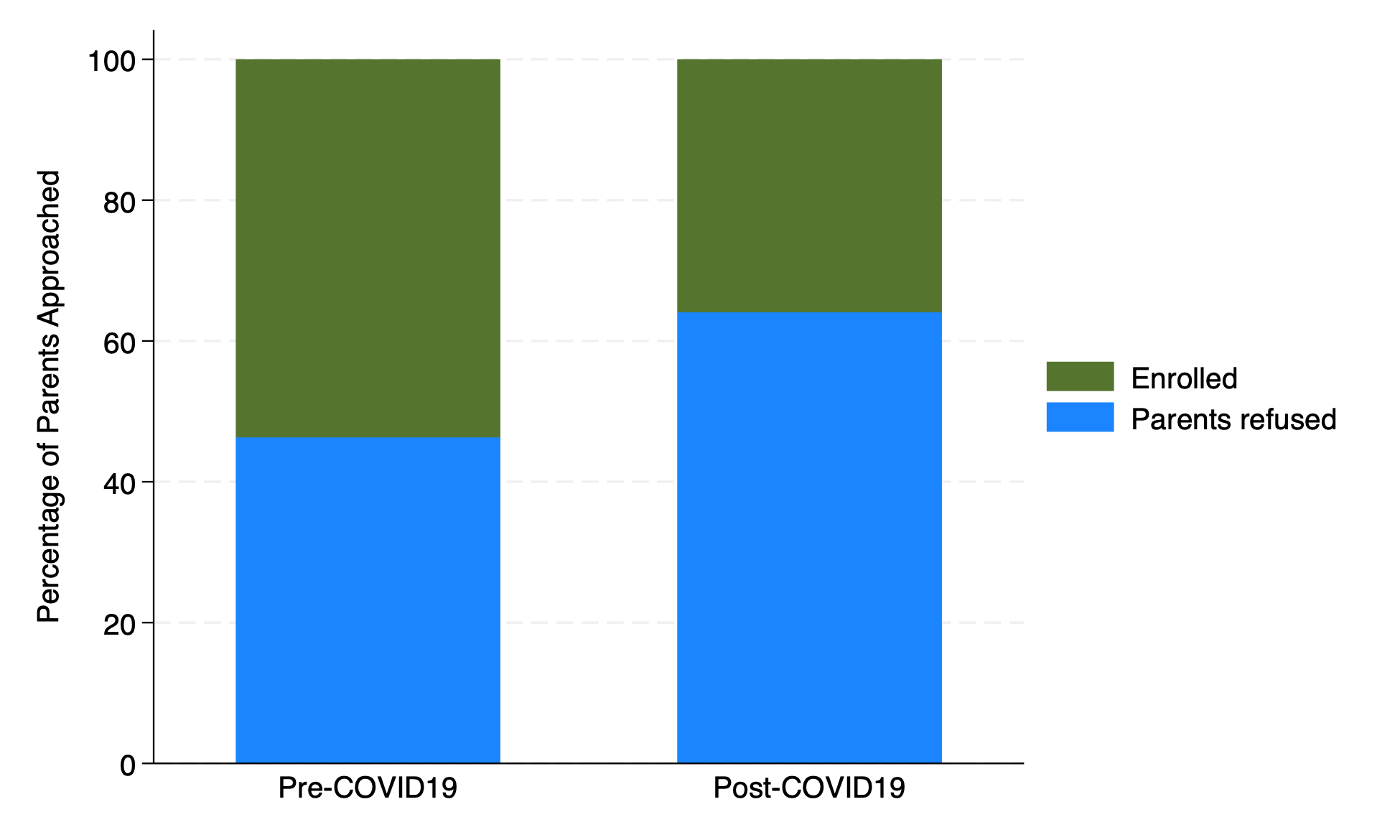 Stacked bar chart of outcomes of parents approached for enrollment. Among these children, the percentage of parental refusal was higher post-COVID19 than pre-COVID19.
Stacked bar chart of outcomes of parents approached for enrollment. Among these children, the percentage of parental refusal was higher post-COVID19 than pre-COVID19.