
Neonatal Quality Improvement 1
Session: Neonatal Quality Improvement 1
 Credit")
Tatyana Kopp, DO (she/her/hers)
Director of Quality and Patient Safety, Inpatient Pediatrics
New York Presbyterian-Queens
Woodmere, New York, United States
.jpg) Percentage of feeding intervals with documented IDF Readiness Scores.
Percentage of feeding intervals with documented IDF Readiness Scores. 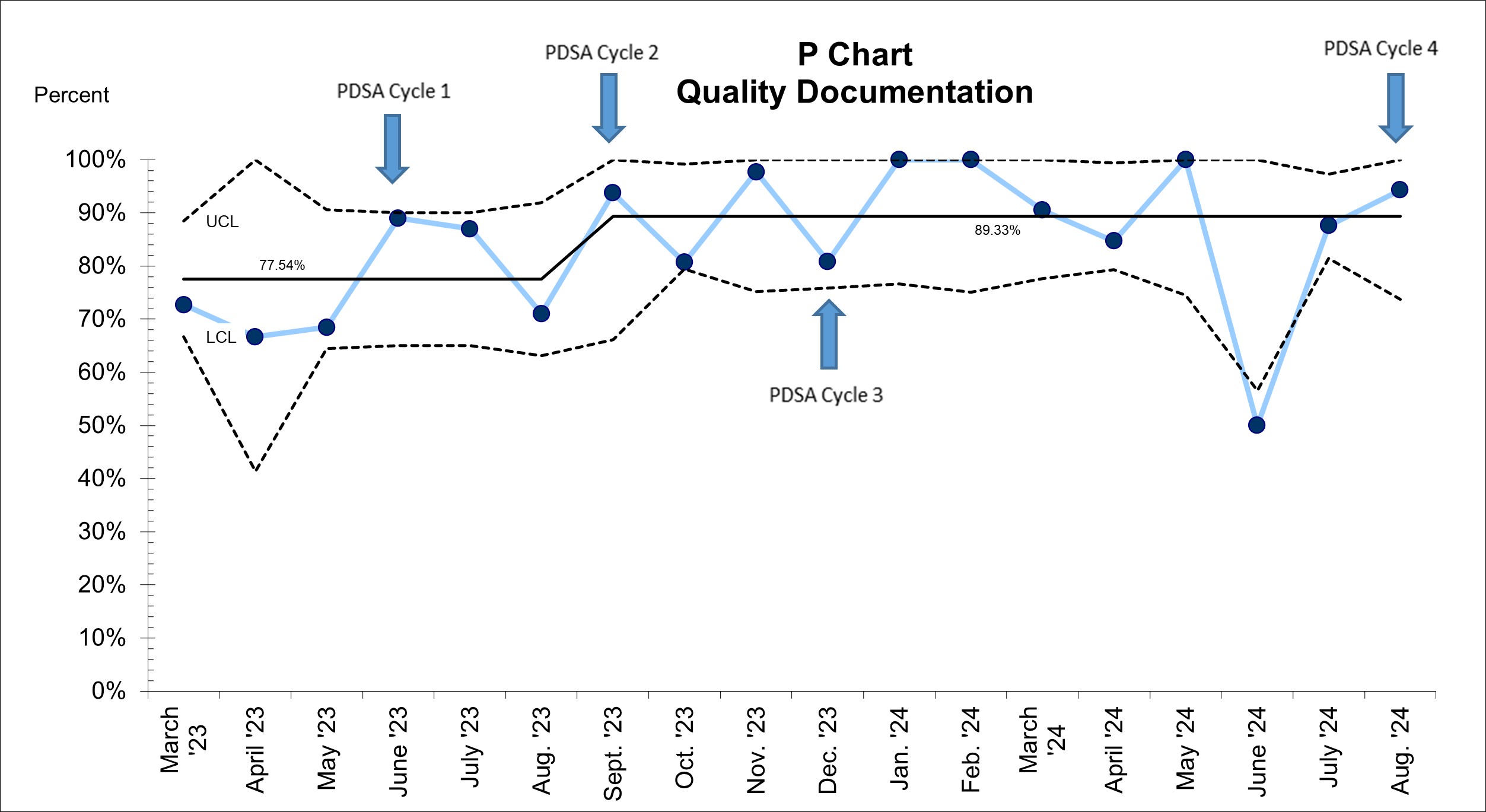 Percentage of oral feeds with documented IDF Quality scores.
Percentage of oral feeds with documented IDF Quality scores. 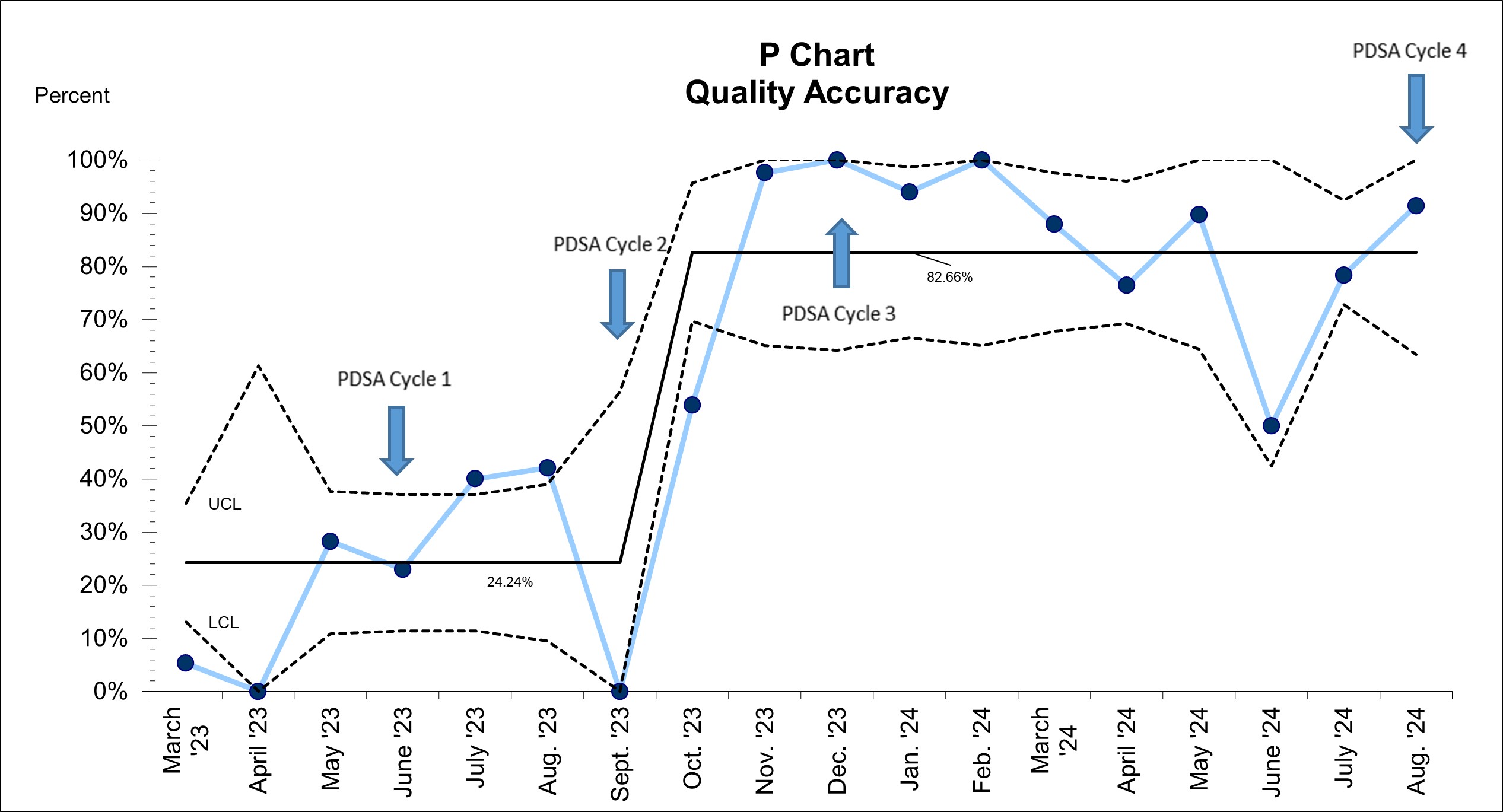 Percentage of documented IDF Quality Scores that were determined and documented accurately.
Percentage of documented IDF Quality Scores that were determined and documented accurately. 