
Neonatal Quality Improvement 1
Session: Neonatal Quality Improvement 1
 Credit")
 photo")
Sandra Leibel, MD MS (she/her/hers)
Associate Professor
University of California, San Diego School of Medicine
San Marcos, California, United States
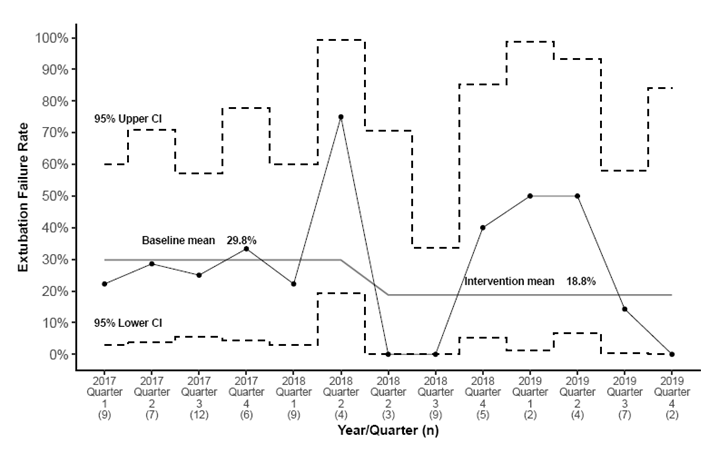 QI intervention begins in 2018 Quarter 2 (second one).
QI intervention begins in 2018 Quarter 2 (second one).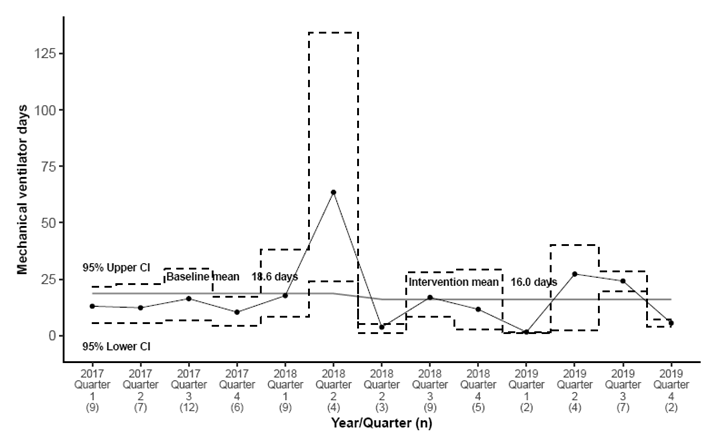 QI intervention begins in 2018 Quarter 2 (second one).
QI intervention begins in 2018 Quarter 2 (second one).