
Neonatal General 4: Novel Technology and Therapies
Session: Neonatal General 4: Novel Technology and Therapies
 photo")
Rina Bao, PhD (she/her/hers)
Instructor
Boston Children's Hospital and Harvard Medical School
Boston, Massachusetts, United States
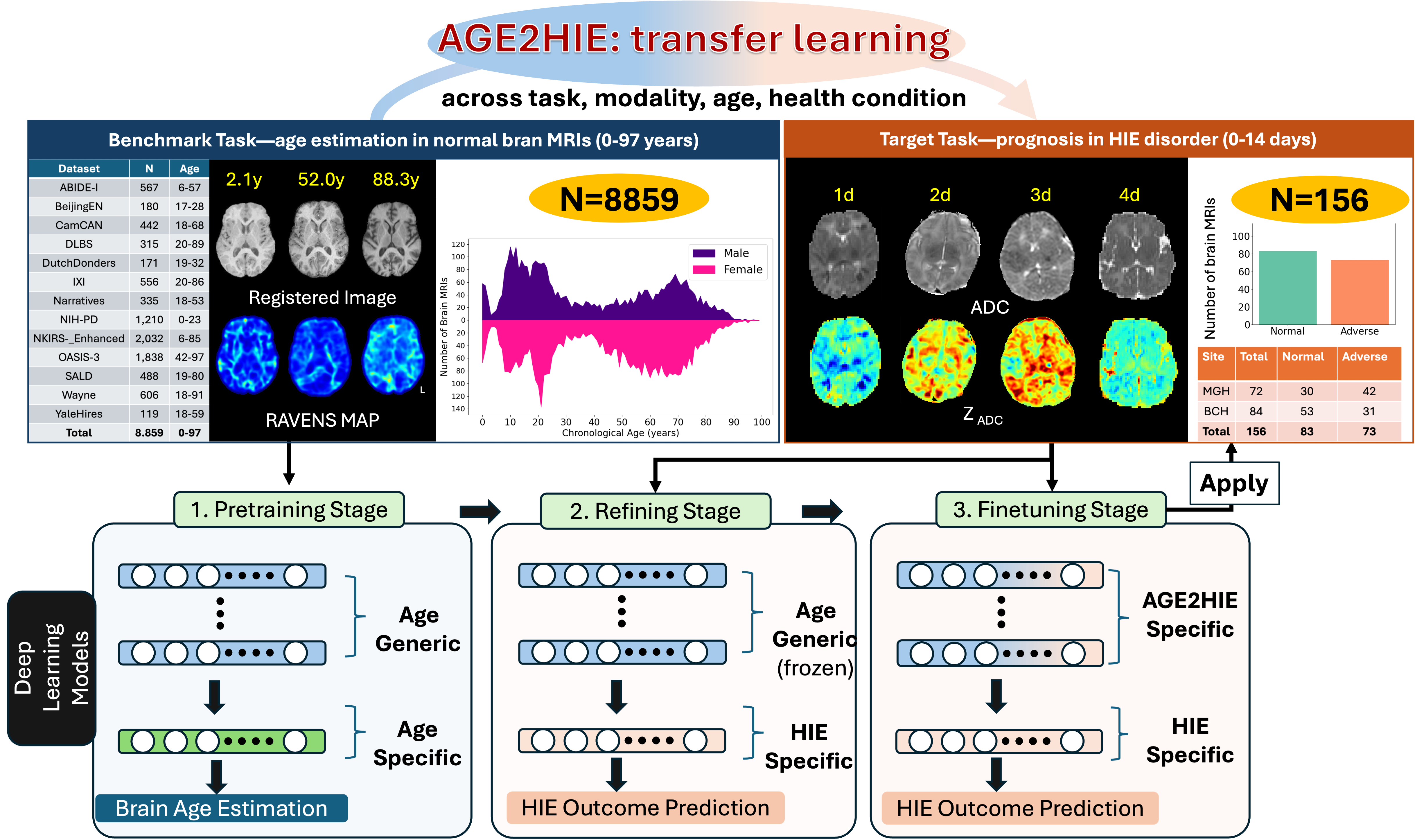 The framework of the proposed AGE2HIE for transferring knowledge learned by deep learning models from brain age estimation (benchmark task, left-upper pannel, with exmaple images and data distribution) with 8,859 samples to HIE outcome prediction (target task, right-upper pannel, with exmaple images and data distribution) with only 156 subjects. The bottom row shows the three stages of transfer learning: 1, Pretraining Stage trains all layers of the model which contains the age generic layers (blue color) and age specific layer (green color); 2, Refining Stage replace the age specific layer to HIE specific layer (orange color) and only trains this HIE specific layer, and 3, Finetuning Stage fine-tunes all layers of the deep learning model to learn the AGE2HIE Specific layers which contains age generic and HIE specific information.
The framework of the proposed AGE2HIE for transferring knowledge learned by deep learning models from brain age estimation (benchmark task, left-upper pannel, with exmaple images and data distribution) with 8,859 samples to HIE outcome prediction (target task, right-upper pannel, with exmaple images and data distribution) with only 156 subjects. The bottom row shows the three stages of transfer learning: 1, Pretraining Stage trains all layers of the model which contains the age generic layers (blue color) and age specific layer (green color); 2, Refining Stage replace the age specific layer to HIE specific layer (orange color) and only trains this HIE specific layer, and 3, Finetuning Stage fine-tunes all layers of the deep learning model to learn the AGE2HIE Specific layers which contains age generic and HIE specific information.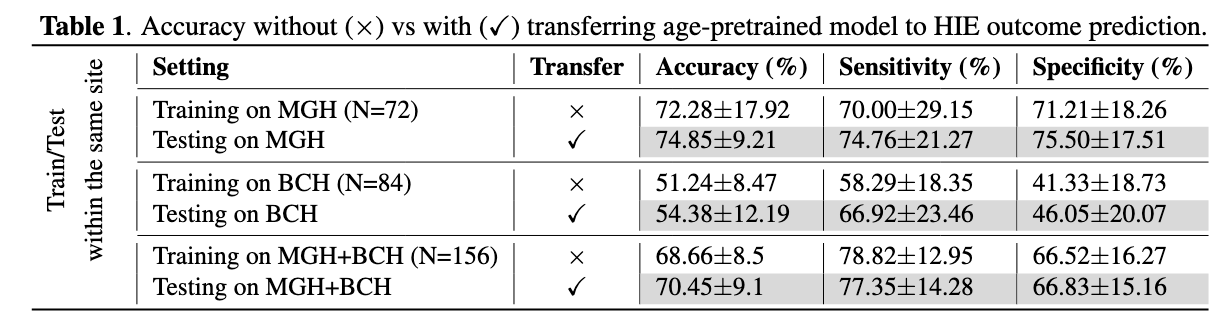 Accuracy without vs with transferring age-pretrained model to HIE outcome prediction.
Accuracy without vs with transferring age-pretrained model to HIE outcome prediction.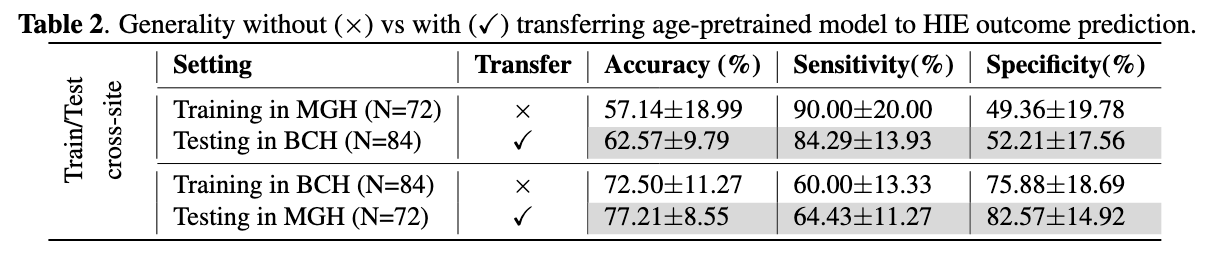 Generality without vs with transferring age-pretrained model to HIE outcome prediction.
Generality without vs with transferring age-pretrained model to HIE outcome prediction.