
Neonatal General 4: Novel Technology and Therapies
Session: Neonatal General 4: Novel Technology and Therapies
 photo")
Vidhi Jhaveri, MD (she/her/hers)
Fellow
University of California, Davis, School of Medicine
Sacramento, California, United States
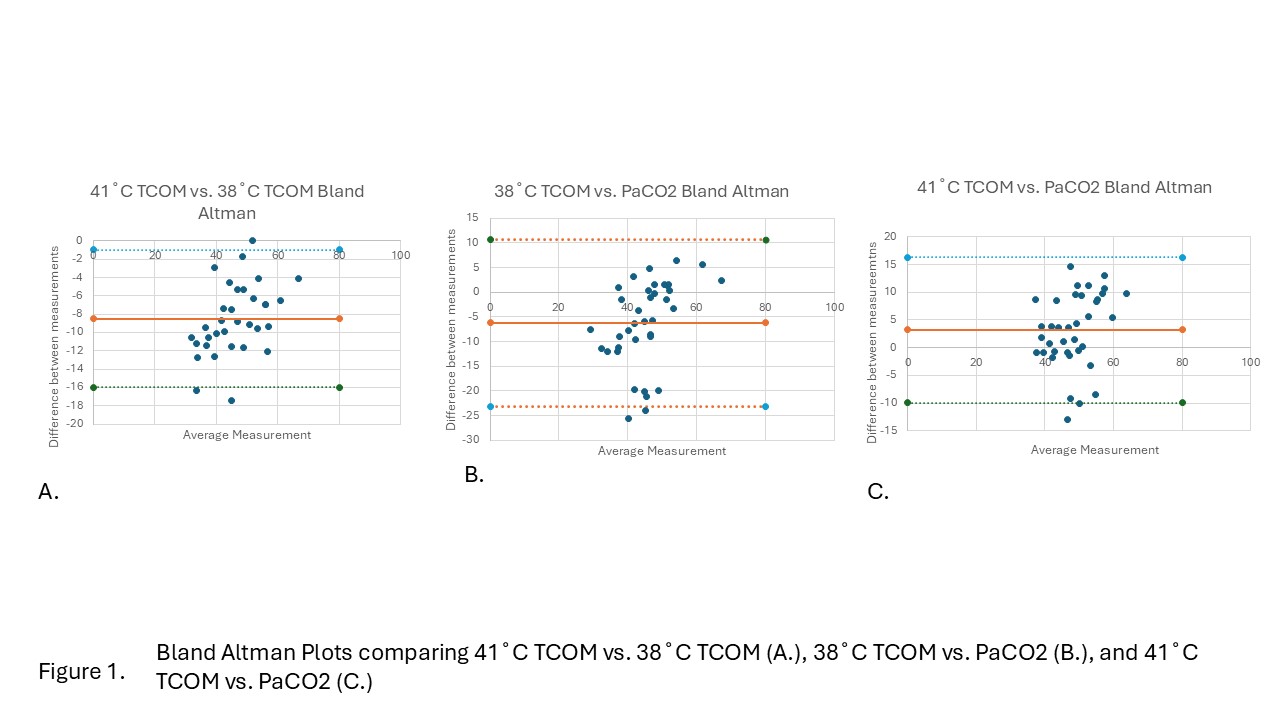 Bland Altman Plots comparing 41˚C TCOM vs. 38˚C TCOM (A.), 38˚C TCOM vs. PaCO2 (B.), and 41˚C TCOM vs. PaCO2 (C.)
Bland Altman Plots comparing 41˚C TCOM vs. 38˚C TCOM (A.), 38˚C TCOM vs. PaCO2 (B.), and 41˚C TCOM vs. PaCO2 (C.) .jpg) Regression analysis comparing 38˚C TcPO2 vs. PaO2 (A.), and 41˚C TcPO2 vs. PaO2 (B.)
Regression analysis comparing 38˚C TcPO2 vs. PaO2 (A.), and 41˚C TcPO2 vs. PaO2 (B.) .jpg) Bland Altman Plots comparing 38˚C TcPO2 vs. PaO2 (A.), and 41˚C TcPO2 vs. PaO2 (B.)
Bland Altman Plots comparing 38˚C TcPO2 vs. PaO2 (A.), and 41˚C TcPO2 vs. PaO2 (B.) 