
Emergency Medicine 4
Session: Emergency Medicine 4
 Credit")
 photo")
Michele McDaniel, MD (she/her/hers)
HS Clinical Associate Professor of Pediatrics
University of California, San Diego School of Medicine
SAN DIEGO, California, United States
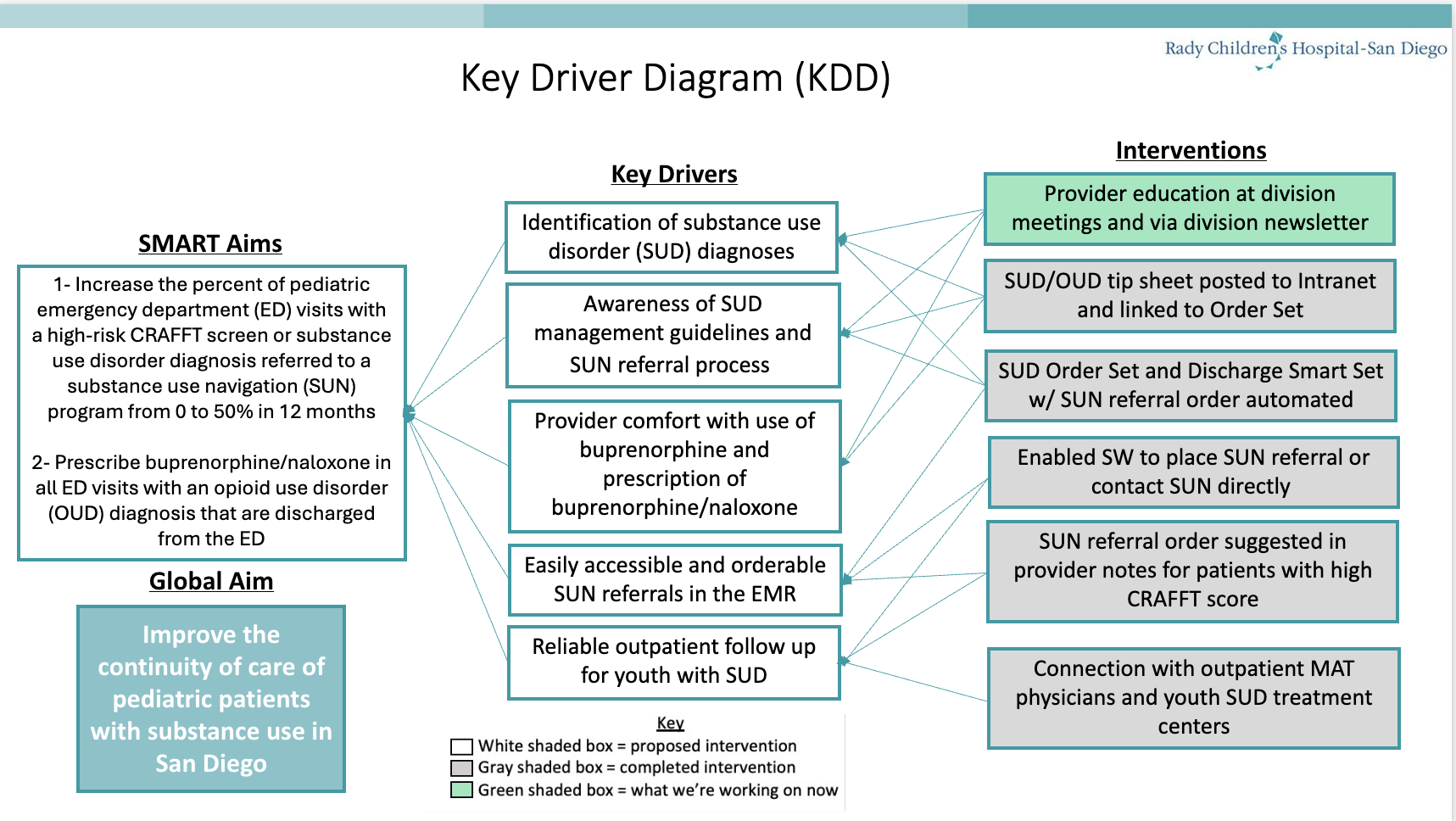 Key Driver Diagram
Key Driver Diagram.png) Control Chart
Control Chart