
Neonatal Nephrology/AKI 2
Session: Neonatal Nephrology/AKI 2
 photo")
Eveline Staub, MD MMed FRACP (she/her/hers)
Unit Director and Staff neonatologist
Royal North Shore Hospital
St Leonards Sydney, New South Wales, Australia
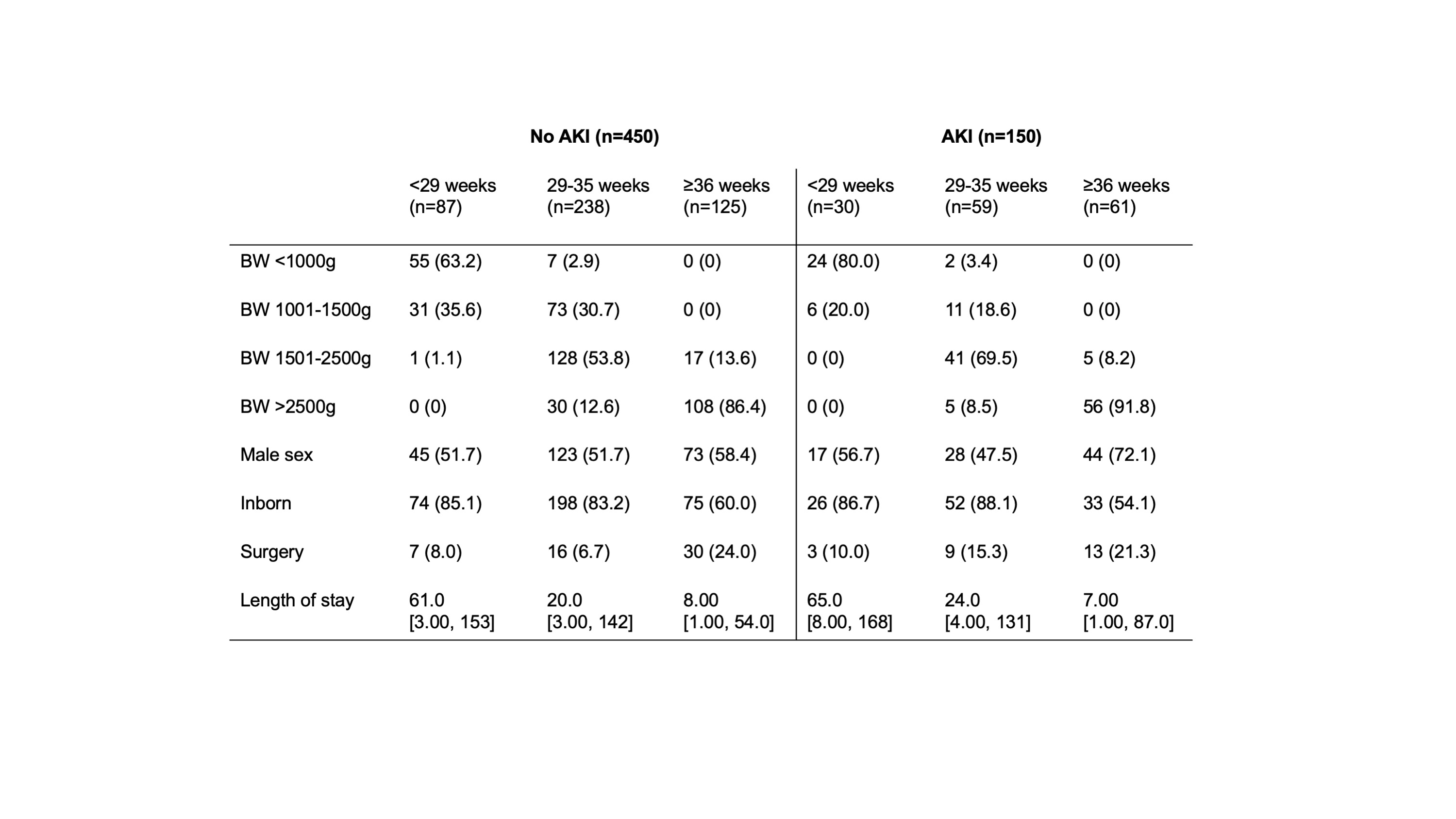 BW: birth weight. Numbers are n with percent in brackets, or median with range in brackets.
BW: birth weight. Numbers are n with percent in brackets, or median with range in brackets.