
Quality Improvement/Patient Safety 5
Session: Quality Improvement/Patient Safety 5
 Credit")
 photo")
Hannah C. Mulvihill, MD (she/her/hers)
Resident Physician
Cohen Children's Medical Center
Manhasset, New York, United States
.png)
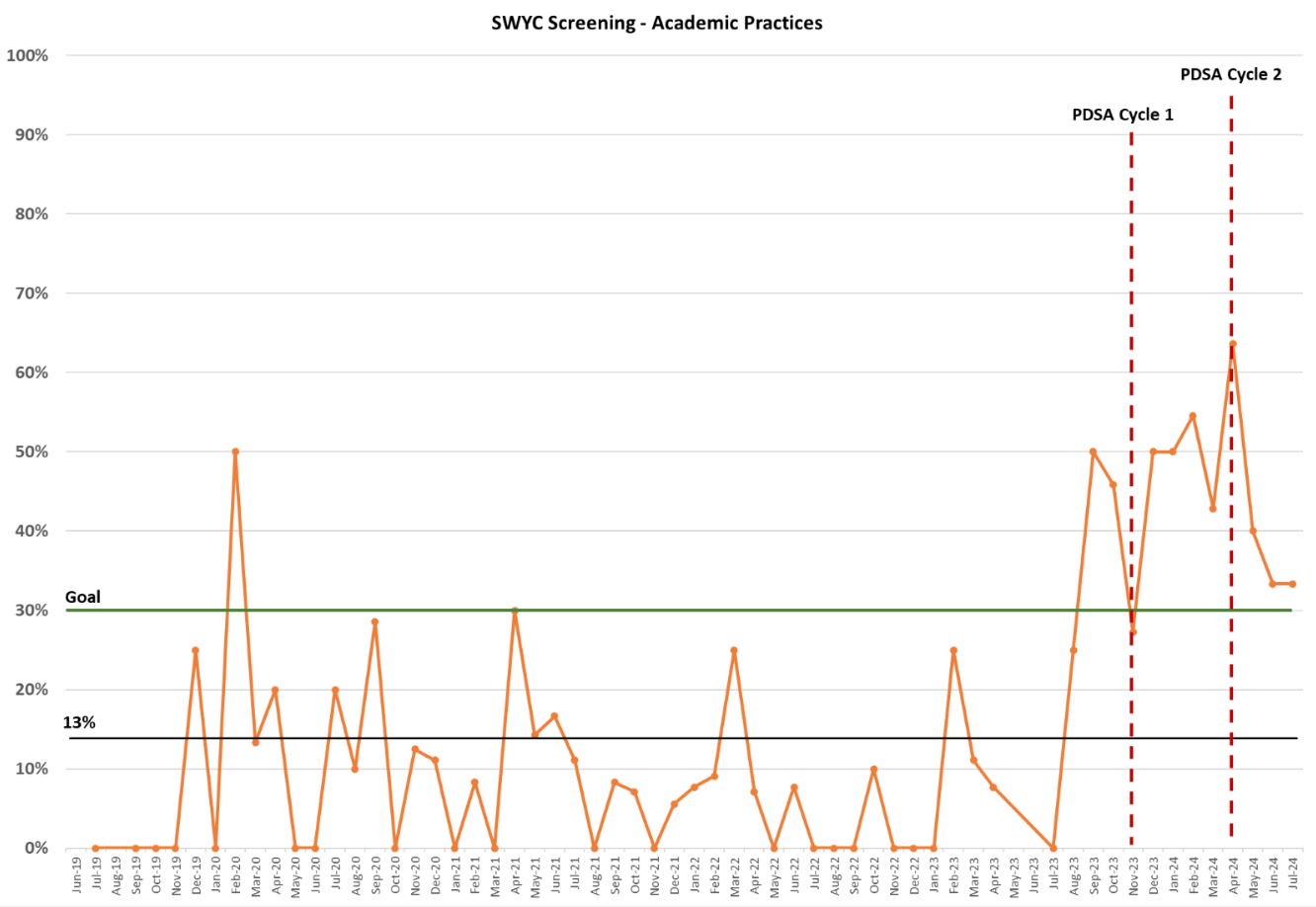 SWYC screening rate depicted over study period for the academic practices, with PDSA cycle 1 (November 2023) and PDSA cycle 2 (April 2024) marked by red dotted line.
SWYC screening rate depicted over study period for the academic practices, with PDSA cycle 1 (November 2023) and PDSA cycle 2 (April 2024) marked by red dotted line..png) SWYC screening rate depicted over study period for both academic and community practices. Average screening rate pre-intervention in academic (13%) and community (26%) practices shown, with goal line in green (30%).
SWYC screening rate depicted over study period for both academic and community practices. Average screening rate pre-intervention in academic (13%) and community (26%) practices shown, with goal line in green (30%).