
Neonatal Quality Improvement 5
Session: Neonatal Quality Improvement 5
 Credit")
 photo")
Alex B. Ruan, MD (he/him/his)
NICU/Clinical Informatics Fellow
Children's Hospital of Philadelphia, Pennsylvania, United States
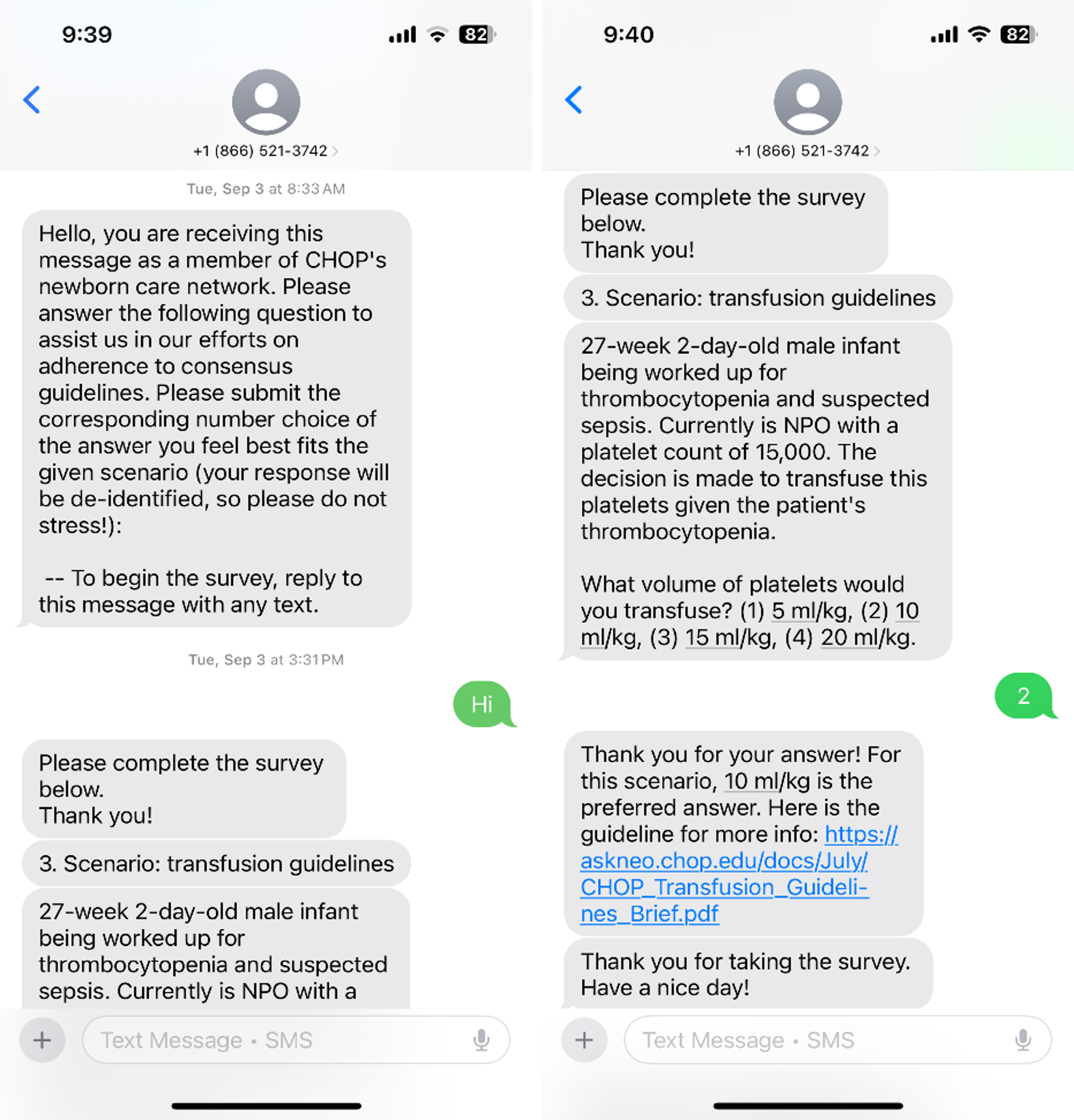 Example of PEAR Tool question with answer and reference link
Example of PEAR Tool question with answer and reference link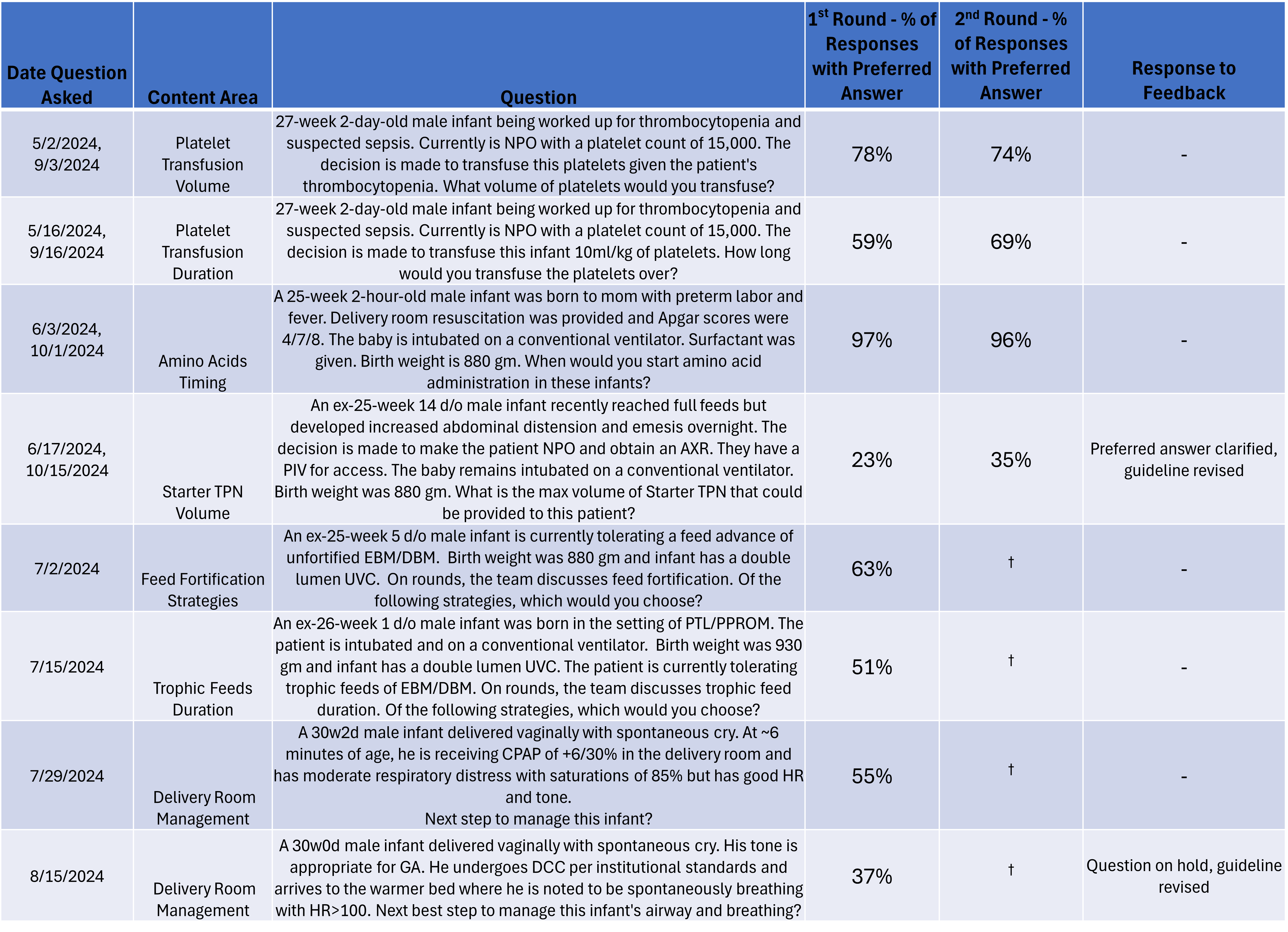 Summary of question content and percent of responses with preferred answer. Data from second round of questions shown, † denotes questions that have not been asked a second time yet. Where applicable, changes made as a result of question feedback are shown.
Summary of question content and percent of responses with preferred answer. Data from second round of questions shown, † denotes questions that have not been asked a second time yet. Where applicable, changes made as a result of question feedback are shown. .png) P-Chart with established trial limits of 12 data points demonstrating response rate for PEAR Tool thus far. Of note, in October 2024 criteria for special cause variation met with two out of three consecutive points near control limit/outer one-third.
P-Chart with established trial limits of 12 data points demonstrating response rate for PEAR Tool thus far. Of note, in October 2024 criteria for special cause variation met with two out of three consecutive points near control limit/outer one-third. 