
Emergency Medicine 6
Session: Emergency Medicine 6
 Credit")

Marsha Dannenberg, MD
Assistant Professor of Pediatrics
Children's Mercy Hospitals and Clinics
Overland Park, Kansas, United States
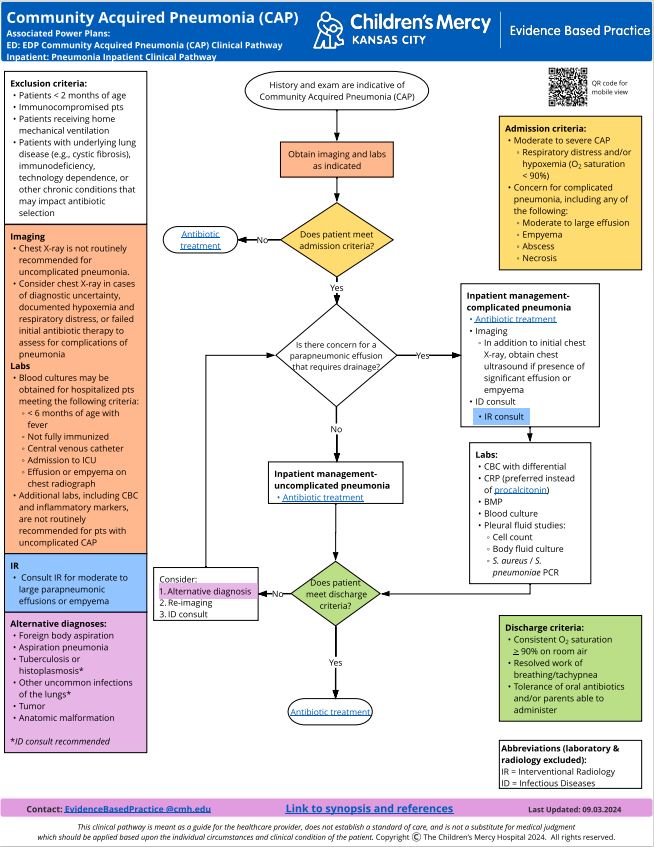 Our institution's clinical pathway for community acquired pneumonia
Our institution's clinical pathway for community acquired pneumonia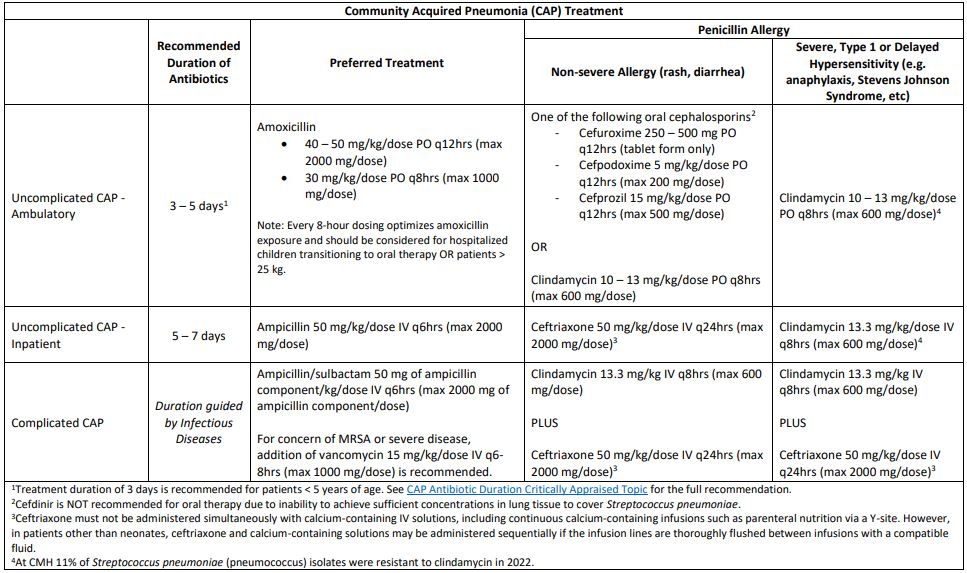 Recommended antibiotic durations for community acquired pneumonia
Recommended antibiotic durations for community acquired pneumonia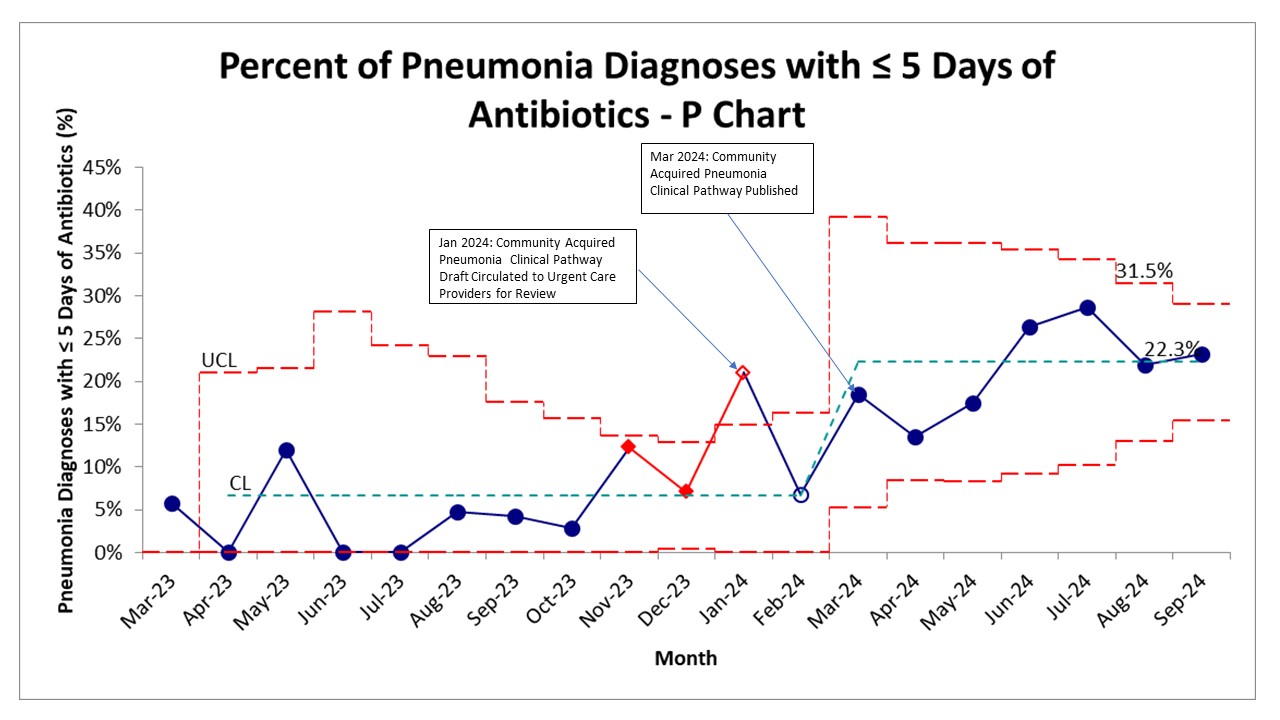 P chart of percent of community acquired pneumonia with antibiotic duration of 5 days or less over time.
P chart of percent of community acquired pneumonia with antibiotic duration of 5 days or less over time.