
Clinical Bioethics
Session: Clinical Bioethics
 photo")
Sarah Porter, MSW, LCSW (she/her/hers)
Manager - Social Work, Clinical Ethics Consultant
Randall Children's Hospital at Legacy Emanuel
Portland, Oregon, United States
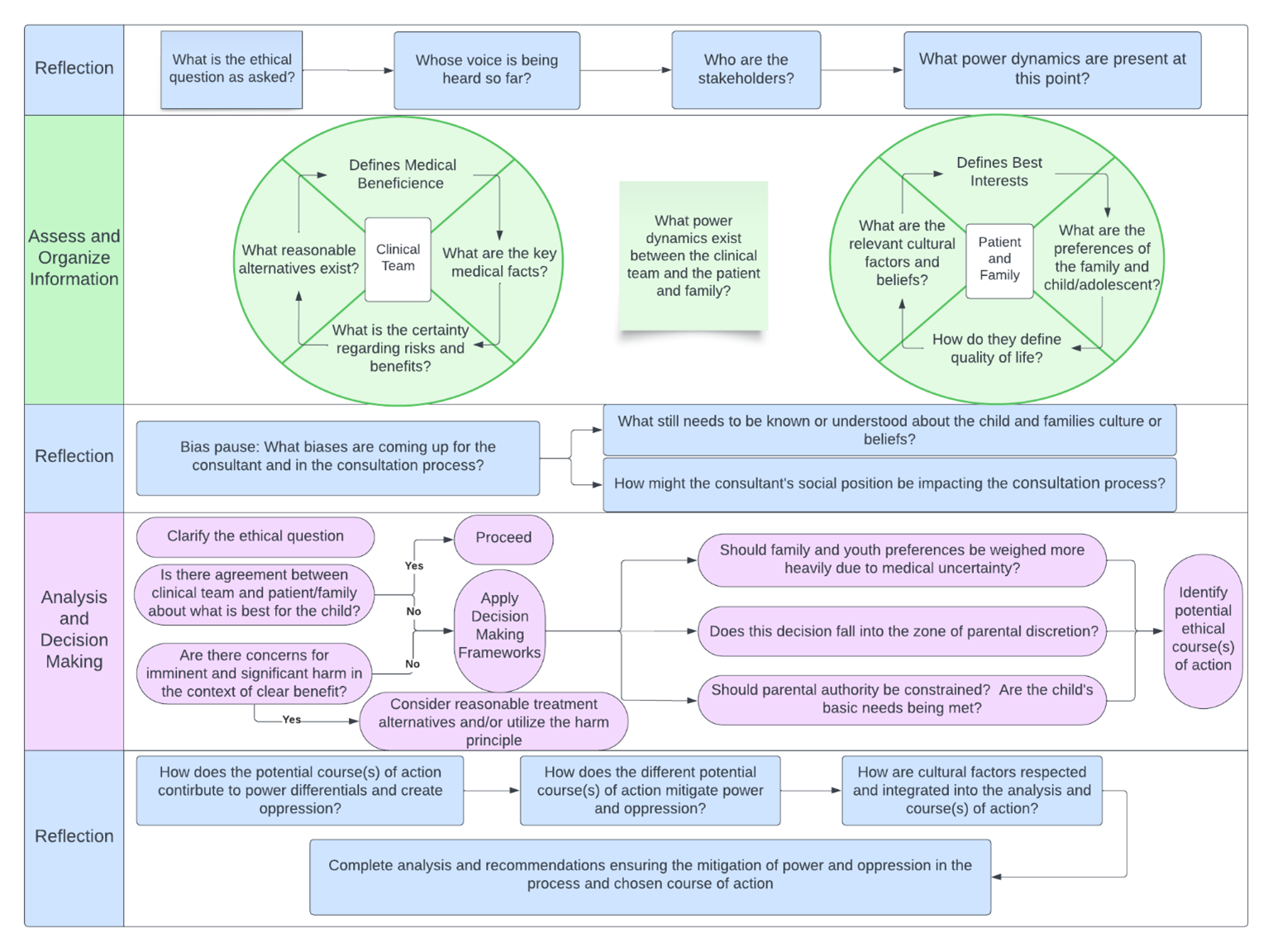 Insertion of an "Ethical Pause and Reflection" into a pediatric bioethics consultation case analysis to mitigate bias, power, and oppression in deriving an ultimate recommendation.
Insertion of an "Ethical Pause and Reflection" into a pediatric bioethics consultation case analysis to mitigate bias, power, and oppression in deriving an ultimate recommendation.