Infectious Diseases 4: Improving antibiotic use
Session: Infectious Diseases 4: Improving antibiotic use
 Credit")
 photo")
Russell J. McCulloh, MD (he/him/his)
Professor
University of Nebraska Medical Center
Omaha, Nebraska, United States
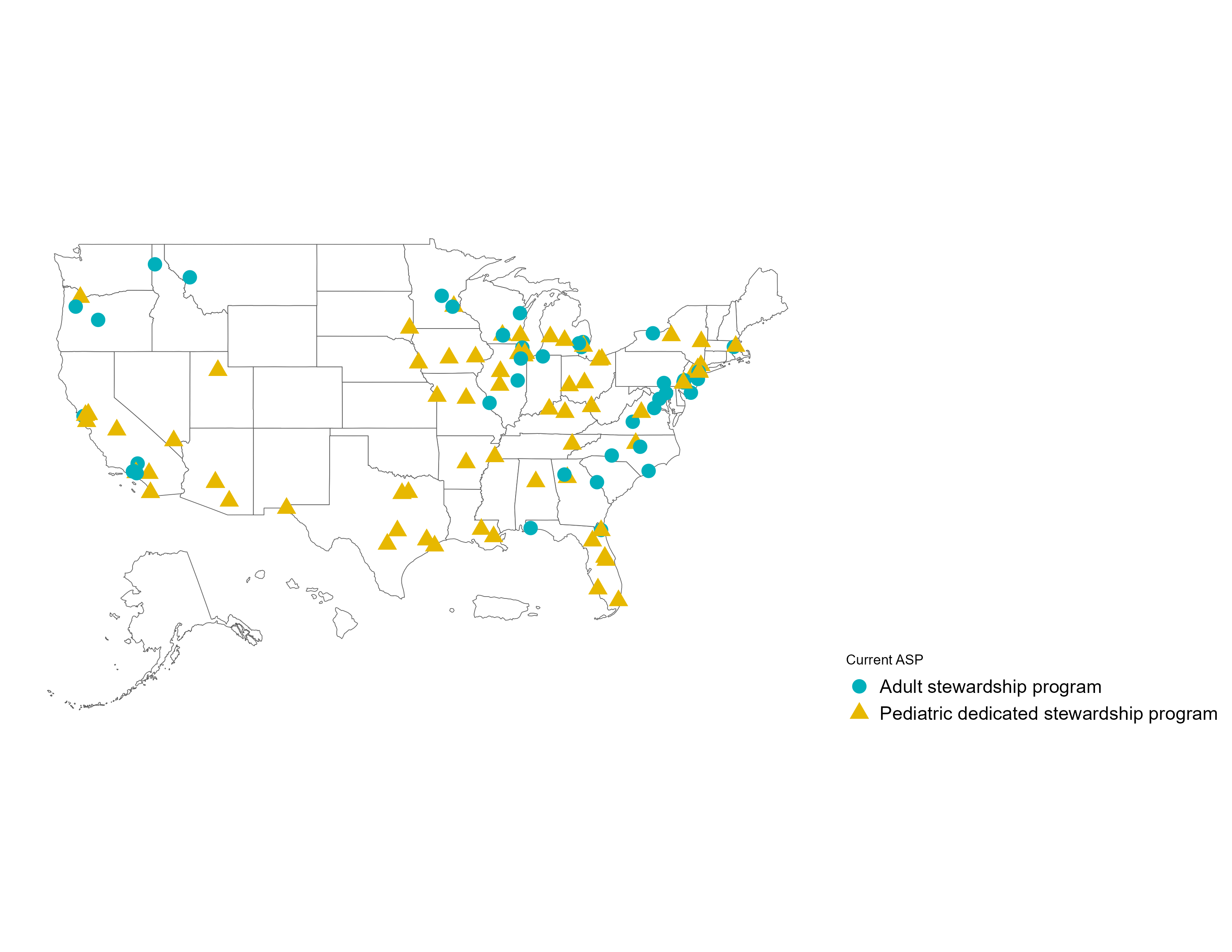 Depicted sites are limited to those that submitted both baseline and post-intervention data.
Depicted sites are limited to those that submitted both baseline and post-intervention data.